Non-Inflammatory Superficial Mycoses
Tinea Nigra Palmaris - Fitzpatrick's Dermatology
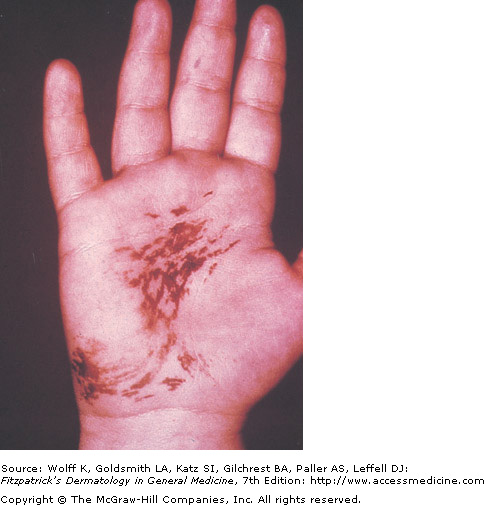
Tinea nigra: Caused by the fungus Hortaea (formerly Exophiala) werneckii, tinea nigra commonly presents as a single brown/grey to green macule or patch that can be velvety in texture. There are no associated symptoms, such as itching. The borders are sharply marginated, and the advancing border may be darker in color than the center. Most cases in North America involve travel to the tropics though cases are seen in the SE US and Texas.
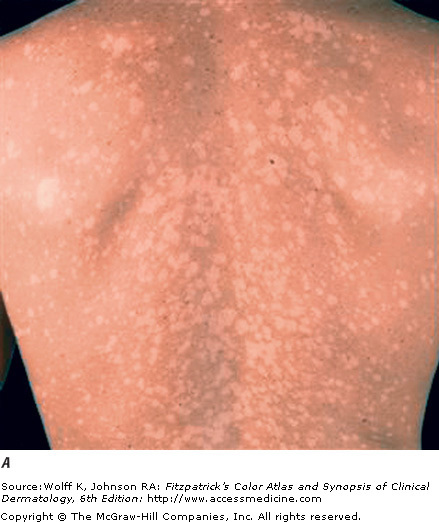
Tinea versicolor: Tinea versicolor, caused by Malassezia furfur, presents with many oval patches or thin plaques. These lesions often group together and become confluent and extensive over the body. The most common areas affected are the upper trunk and shoulders. The most common colors are tan (hypopigmented) and brown (hyperpigmented). Tinea versicolor is not associated with any serious symptoms, and the main patient concern is cosmetic appearance.
Tinea versicolor: Tinea versicolor, caused by Malassezia furfur, presents with many oval patches or thin plaques. These lesions often group together and become confluent and extensive over the body. The most common areas affected are the upper trunk and shoulders. The most common colors are tan (hypopigmented) and brown (hyperpigmented). Tinea versicolor is not associated with any serious symptoms, and the main patient concern is cosmetic appearance.
 Tinea Versicolor - Fitzpatrick's Dermatology |
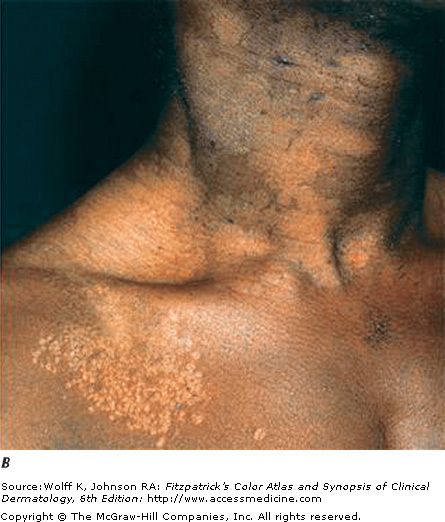 Tinea Versicolor in African Skin - FItzpatrick's Dermatology |
Dermatophytoses

Tinea Corporis
Dermatophytoses are fungal infections caused by fungi from the genera Microsporum, Trichophyton, and Epidermophyton. These "dermatophytes" are unique because they have the ability to invade and colonize keratinized tissue, such as hair, skin, and nails. They produce enzymes called keratinases that break down keratin tissue, allowing for their invasion. Many host factors are involved in limiting the spread of dermatophyte infection, including the patient's genetic predisposition, immune status, and other underlying diseases.
Tinea corporis: This dermatophyte infection invovles the trunk and extremities, and is generally limited to the stratum corneum. The most common cause is the organism Trichophyton rubrum followed by T.mentagrophytes. Risk factors for this infection include an infected pet, exposure to tinea capitis or tinea pedis, exposure through exercise or contact sports, especialy wrestling, and any close or shared quarters. Infection spreads in a centrifugal manner with central clearing often noted, leading to annular lesions of different sizes. Many lesions are scaly, and pustules are contained within the active border. The symptoms associated with tinea corporis are burning and pruritis (itching).
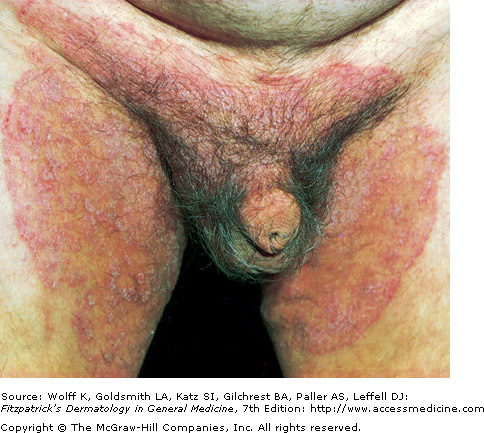
Tinea cruris: A dermatophyte infection of the inguinal region, especially the upper thighs, this condition is more common in men and in obese patients. Classic lesions are well demarcated with a raised, erythematous, scaly advancing border, which may contain pustules or vesicles. Tinea pedis should be co-treated since it may be the source of infection. The scrotum is typically spared in these infections, and if the scrotum is involved, one should consider candidiasis.
Tinea capitis: This infection is common in the scalp of children, and does not occur frequently in adults. It has a wide range of presentations, from a non-inflammatory scaling to a severe pustular eruption with hair loss. Sharing or reusing without washing of hats, caps, and brushes can be problematic.
There are many other conditions that caused scalp scaling and hair loss, however fungal infections should be included on the differential as they are easy to effectively treat. This disease is contagious so family members should be screened for tinea capitis.
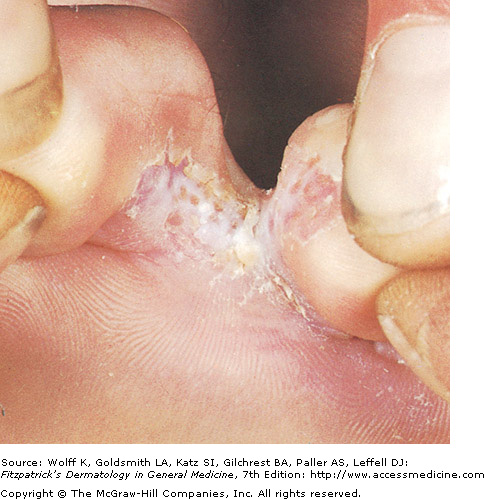
Tinea pedis: A dermatophyte infection of the soles of the feet and interdigital spaces, tinea pedis is a common condition that is thought to be associated with walking barefoot in gyms, locker rooms, and public places. There are four major types of tinea pedis: moccasin, interdigital, inflammatory, and ulcerative. The most common type, interdigital, is associated with erythema, scaling, fissures, and maceration in the web spaces. Itching is common, and the infection can extend to the sole of the foot.
Tinea corporis: This dermatophyte infection invovles the trunk and extremities, and is generally limited to the stratum corneum. The most common cause is the organism Trichophyton rubrum followed by T.mentagrophytes. Risk factors for this infection include an infected pet, exposure to tinea capitis or tinea pedis, exposure through exercise or contact sports, especialy wrestling, and any close or shared quarters. Infection spreads in a centrifugal manner with central clearing often noted, leading to annular lesions of different sizes. Many lesions are scaly, and pustules are contained within the active border. The symptoms associated with tinea corporis are burning and pruritis (itching).
Tinea cruris: A dermatophyte infection of the inguinal region, especially the upper thighs, this condition is more common in men and in obese patients. Classic lesions are well demarcated with a raised, erythematous, scaly advancing border, which may contain pustules or vesicles. Tinea pedis should be co-treated since it may be the source of infection. The scrotum is typically spared in these infections, and if the scrotum is involved, one should consider candidiasis.
Tinea capitis: This infection is common in the scalp of children, and does not occur frequently in adults. It has a wide range of presentations, from a non-inflammatory scaling to a severe pustular eruption with hair loss. Sharing or reusing without washing of hats, caps, and brushes can be problematic.
There are many other conditions that caused scalp scaling and hair loss, however fungal infections should be included on the differential as they are easy to effectively treat. This disease is contagious so family members should be screened for tinea capitis.
Tinea pedis: A dermatophyte infection of the soles of the feet and interdigital spaces, tinea pedis is a common condition that is thought to be associated with walking barefoot in gyms, locker rooms, and public places. There are four major types of tinea pedis: moccasin, interdigital, inflammatory, and ulcerative. The most common type, interdigital, is associated with erythema, scaling, fissures, and maceration in the web spaces. Itching is common, and the infection can extend to the sole of the foot.
|
|


Cutaneous Candidiasis
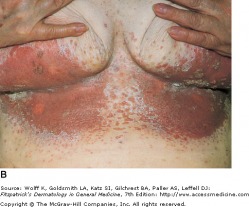
Cutaneous Candidiasis with Satellite Lesions
This yeast infection presents as erythematous to slightly erosive patches that are accompanied by satellite pustules. Caused most frequently by Candida albicans or Candida tropicalis, the most common sites of involvement include areas of skin folds and creases, the scrotum, and diaper areas in babies. Candidiasis can also be seen in conjunction with other conditions, such as superimposed on seborrheic dermatitis or psoriasis. Diagnosis is made clinically, or by microscopy with a KOH slide preparation and potentially by culture. Topicals are usually effective therapies but with more advanced or erosive findings, an oral is preferred. Local skin care is also necessary with increased moisture control and cooler environment if possible.
Sporotrichosis

Sporotrichosis - Fitzpatrick's Dermatology
Also known as rose gardener's disease, sporotrichosis is a subcutaneous mycosis caused by Sporothrix schenckii. The most common presentation is a primary innoculation site manifesting as a single papule, commonly on the hand or foot. The lesion then becomes eroded or ulcerated and may drain purulent fluid, although it is typically not painful. Additional nodules then appear following the pattern of lymphatic drainage from the initial lesion. Lymphatic vessels can become fibrosed.
Histoplasmosis

Disseminated Histoplasmosis - Fitzpatrick's
Histoplasmosis is endemic to the central and southeast regions of the United States, and typically does not cause symptoms in immunocompetent individuals. Bird and bat droppings are resevoirs of Histoplasma capsulatum, making caves and chicken coops high risk areas. Up to 90 percent of the population in endemic areas tests positive in histoplasmin skin testing. When a patient is immunocompromised, such as in HIV infection, histoplasmosis becomes a serious respiratory disease that can disseminated and spread throughout the body. Oral ulcers are the most common manifestation, and are seen in half of immunocompetent patients. Immunocompromised patients may present with mucocutaneous erosions or ulcers, along with many erythematous pauples or nodules with scales or crust. Synonyms for histoplasmosis include Ohio Valley disease and Darling's disease.
Blastomycosis

Blastomycosis - Fitzpatrick's Dermatology
Caused by the organism Blastomyces dermatitidis, blastomycosis is endemic to the southeast. Soil is the most likely source of infections, and occupations with outdoor exposure should raise suspicion. The common presentations are papulopustules and verrucous plaques with scale-curst and pustules on the border. With central ulceration, these lesions can look very similar to pyoderma gangrenosum.
Histological examination with PAS or methenamine silver stain will allow the visualization of characteristic broad budding with double contoured walls. The respiratory system is typically first infected, with secondary cutaneous findings. In some patients, respiratory symptoms may be subclinical, and skin lesions may be the first sign of disease.
Histological examination with PAS or methenamine silver stain will allow the visualization of characteristic broad budding with double contoured walls. The respiratory system is typically first infected, with secondary cutaneous findings. In some patients, respiratory symptoms may be subclinical, and skin lesions may be the first sign of disease.
