Top Common Conditions
The purpose of this section is to inform the medical student of the most common conditions dermatologists diagnose and treat on a daily basis. While this list is not comprehensive, it presents the major diseases medical students should be familiar with upon graduation. This is invaluable for all medical students as common skin conditions prompt many office visits. Multiple photos are given for many conditions to show the variability of the skin lesions in a particular disorder.
Acne
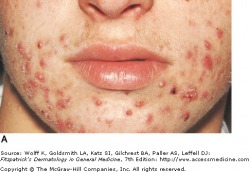
Acne Vulgaris - Mild to Moderate
Acne vulgaris is a disorder of the pilosebaceous unit, seen primarily in adolescents and young adults. It often presents with pleomorphic lesions, including comedomes, papules, pustules, and nodules. While acne can be self-limiting, life long consequences such as scarring can remain. Acne is most often intially problematic during puberty, with the greatest prevalence in the mid to late teen years. It may persist, particularly in women, throughout the third decade of life and beyond.
Acne is primarily found on the face, back, chest, and shoulders. Many different types of lesions can be found, and they can be either inflammatory or non-inflammatory. The non-inflammatory lesions are comedos, which can be open (blackheads, flat or slightly raised with a central dark impaction) or closed (whiteheads, pale, elevated small papules). Inflammatory lesions can vary greatly, ranging from small erythematous papules to large, tender, fluctuant cysts.
A variety of treatments are available for acne vulgaris. Topical OTC products include benzoyl peroxide and salicyclic acid. Prescription topical drugs include the retinoid(tretinoin,adalalene, and tazarotene) family of anti-inflammatory comedolytics,topical antibiotics (erythromycin and clindamycin), and azelaic acid. Systemic treatments can include tetracyclines, macrolides, trimethopim-sulfamethoxazole, hormonal therapy, and isotretinoin (Accutane).
Acne is primarily found on the face, back, chest, and shoulders. Many different types of lesions can be found, and they can be either inflammatory or non-inflammatory. The non-inflammatory lesions are comedos, which can be open (blackheads, flat or slightly raised with a central dark impaction) or closed (whiteheads, pale, elevated small papules). Inflammatory lesions can vary greatly, ranging from small erythematous papules to large, tender, fluctuant cysts.
A variety of treatments are available for acne vulgaris. Topical OTC products include benzoyl peroxide and salicyclic acid. Prescription topical drugs include the retinoid(tretinoin,adalalene, and tazarotene) family of anti-inflammatory comedolytics,topical antibiotics (erythromycin and clindamycin), and azelaic acid. Systemic treatments can include tetracyclines, macrolides, trimethopim-sulfamethoxazole, hormonal therapy, and isotretinoin (Accutane).
 Acne Pathogenesis |
 Severe, Nodular Acne Vulgaris |
Rosacea

Papulopustular Rosacea
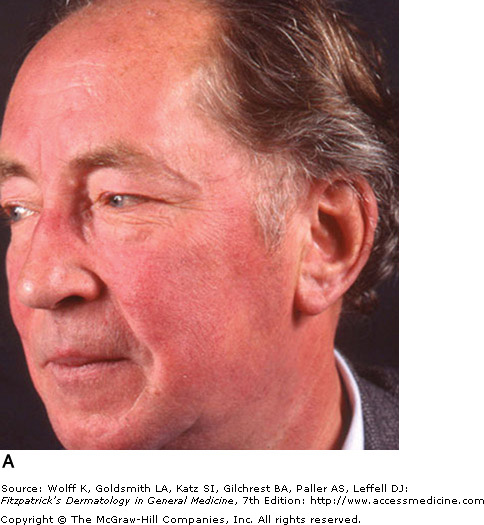
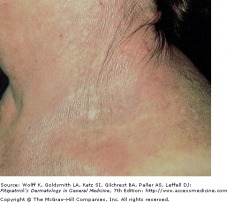
Rosacea is a chronic erythematous inflammation of the cheeks, nose, chin, forehead, and eyelids. This occurs due to the prominence of superficial blood vessels in the face, and can be triggered by environmental, emotional, and hormonal events that promote flushing.
Erythematotelangiectatic rosacea (ETR) is a persistent facial erythema and flushing, with telangiectases, central face edema, burning/stinging, roughness or scaling, or any combination of these symptoms. Papulopustular rosacea (PPR) presents as a persistent central face erythema with papules and pustules. Burning and stinging can occur in PPR, but it is more common to find this symptom in ETR.
The differential diagnosis for rosacea is large and complex, as many other conditions can mimic the signs of rosacea. Systemic diseases include polycythemia vera, mastocytosis, carcinoid syndrome, and connective tissue disorders, such as systemic lupus erythematosus. Neurologic conditions, such as brain tumors and spinal cord lesions can cause flushing, and certain drugs can induce flushing, including all vasodilators, calcium channel blockers, niacin, morphine, and systemic steroids.
Erythematotelangiectatic rosacea (ETR) is a persistent facial erythema and flushing, with telangiectases, central face edema, burning/stinging, roughness or scaling, or any combination of these symptoms. Papulopustular rosacea (PPR) presents as a persistent central face erythema with papules and pustules. Burning and stinging can occur in PPR, but it is more common to find this symptom in ETR.
The differential diagnosis for rosacea is large and complex, as many other conditions can mimic the signs of rosacea. Systemic diseases include polycythemia vera, mastocytosis, carcinoid syndrome, and connective tissue disorders, such as systemic lupus erythematosus. Neurologic conditions, such as brain tumors and spinal cord lesions can cause flushing, and certain drugs can induce flushing, including all vasodilators, calcium channel blockers, niacin, morphine, and systemic steroids.
 ETR Rosacea |
 Close-up ETR Rosacea - Note the telangiectasias and few pustules |
Atopic Dermatitis
Prurigo Papules of Atopic Dermatitis
Atopic dermatitis (atopic eczema) is a chronic relapsing disease associated with abnormalities in skin barrier function and allergen sensitization. There is no definitive single feature or laboratory test available, however the following features have been described:
Major Features:
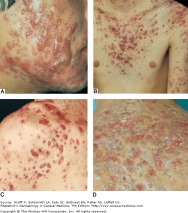
Cutaneous lesions found in atopic dermatitis can vary greatly from patient to patient, are usually worse in the late evening, and involve prurigo papules, lichenification, and eczematous skin lesions. Acute lesions are intensely pruritic, and characterized by erythematous papules with excoriation, vesicles over erythematous skin, and serous exudates. Subacute dermatitis is associated with erythematous, scaling papules. Chronic atopic dermatitis is characterized by thickened plaques of skin, lichenification, and fibrotic papules. All three stages may be present on one individual, and at all stages, the skin is noted to have a dry, lackluster appearance.
Major Features:
- -Pruritis
- -Rash on face and/or extensors in children
- -Lichenification in flexural areas in older children
- -Tendency towards chronic dermatitis
-Personal or family history of asthma, allergic rhinitis, or atopic dermatitis
-Immunoglobulin E reactivity
Cutaneous lesions found in atopic dermatitis can vary greatly from patient to patient, are usually worse in the late evening, and involve prurigo papules, lichenification, and eczematous skin lesions. Acute lesions are intensely pruritic, and characterized by erythematous papules with excoriation, vesicles over erythematous skin, and serous exudates. Subacute dermatitis is associated with erythematous, scaling papules. Chronic atopic dermatitis is characterized by thickened plaques of skin, lichenification, and fibrotic papules. All three stages may be present on one individual, and at all stages, the skin is noted to have a dry, lackluster appearance.
|
|



Seborrheic Dermatitis

Seborrheic Dermatitis of Central Face
Seborrheic dermatitis is a common chronic papulosquamous condition associated with increased sebum production. The areas affected are those with high concentrations of sebaceous follicles, including the scalp, ears, face, and certain areas of the trunk. Skin is pink, edematous, and covered in yellow-brown crusts and scales that are greasy or oily. Inflammatory seborrheic dermatitis is common in HIV/AIDS patients, and the diagnosis should be considered in high-risk patients or in cases where the dermatitis is resistant to treatment. Neurological conditions as Parkinson's also may have refractory seborrhea.
Lesions can be pruritic, especially on the scalp and ears. The condition lasts for years to decades, with typical improvement in the warmer months. Seborrheic dermatitis is highly variable in its presentation, and may be limited to specific areas or more widespread.
Lesions can be pruritic, especially on the scalp and ears. The condition lasts for years to decades, with typical improvement in the warmer months. Seborrheic dermatitis is highly variable in its presentation, and may be limited to specific areas or more widespread.
Contact Dermatitis
Allergic Contact Dermatitis
Contact dermatitis comes in two general varieties: allergic and irritant. Allergic contact dermatitis can be triggered by over 3700 plus known allergens, and irritant contact dermatitis involves contact with an agent that is inherently toxic to human skin, often due to occupational exposure.
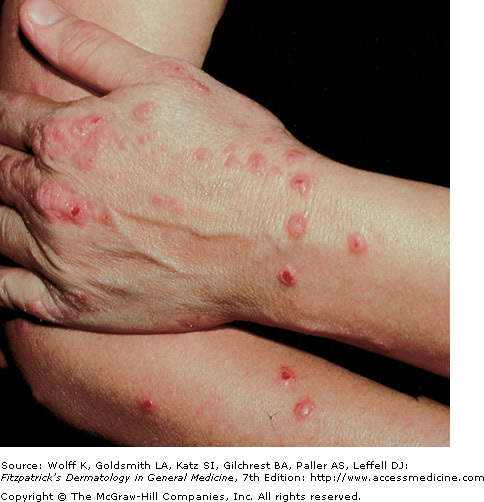
Allergic contact dermatitis is the presentation of delayed-type hypersensitivity responses to exogenous agents. Generally, once a patient is sensitized, the lesion moves from erythema to edema to papulovesiculation. It is also important to note allergic contact dermatitis usually occurs in the distribution of exposure. A good example is poison ivy exposure in which you expect to see a linear edematous plaque where the plant or a branch with the plant's urushiol touched the skin. Other exposure occurs via pets or handling clothing or firewood that has been exposed. The amount of antigen also determines the rate and severity of reaction. In cases of persistent exposure, lichenification and scaling occur.
Irritant contact dermatitis is most often associated with some sort of occupational exposure, and is caused by a chemical, physical, or biological agent that is toxic to skin. Unlike allergic contact dermatitis, no previous exposure is necessary to illicit a reaction. In atopic dermatitis, skin barrier function is compromised, putting these patients at higher risk for irritant contact dermatitis. The goal of the clinician should be identification and avoidance of the causative irritant. Patch testing is available to distinguish between allergic and irritant reactions.
Allergic contact dermatitis is the presentation of delayed-type hypersensitivity responses to exogenous agents. Generally, once a patient is sensitized, the lesion moves from erythema to edema to papulovesiculation. It is also important to note allergic contact dermatitis usually occurs in the distribution of exposure. A good example is poison ivy exposure in which you expect to see a linear edematous plaque where the plant or a branch with the plant's urushiol touched the skin. Other exposure occurs via pets or handling clothing or firewood that has been exposed. The amount of antigen also determines the rate and severity of reaction. In cases of persistent exposure, lichenification and scaling occur.
Irritant contact dermatitis is most often associated with some sort of occupational exposure, and is caused by a chemical, physical, or biological agent that is toxic to skin. Unlike allergic contact dermatitis, no previous exposure is necessary to illicit a reaction. In atopic dermatitis, skin barrier function is compromised, putting these patients at higher risk for irritant contact dermatitis. The goal of the clinician should be identification and avoidance of the causative irritant. Patch testing is available to distinguish between allergic and irritant reactions.
|
 Irritant Contact Dermatitis due to toilet seat - DermAtlas |


Psoriasis
Psoriasis Lesion and Auspitz Sign
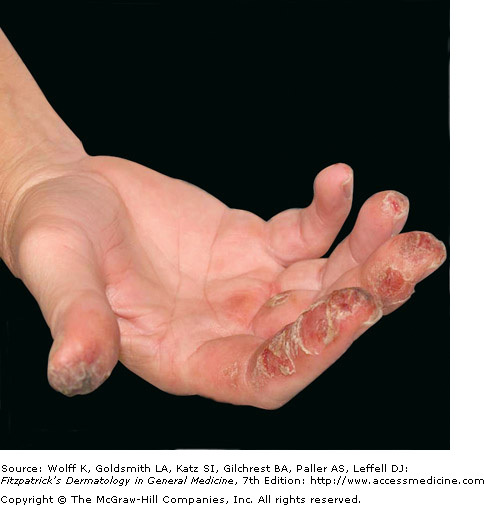
Psoriasis, affecting about 2% of the world's population, is a chronic disease with a genetic component in conjunction with triggering environmental factors. The classic lesion is a well-demarcated, raised, red plaque with a white scaly surface. Lesions vary in size from pinpoint papules to large plaques covering significant areas of the body. Underneath the white scale, the lesion is glossy and erythematous, and bleeding occurs with the removal of the scale due to trauma to the dilated capillaries (Auspitz sign). Psoriatic arthritis may occur and has a strong genetic component.
Psoriasis vulgaris is seen in approximately 90 percent of psoriasis patients. Red, scaly plaques are located in extensor areas of the extremities, especially the elbows and knees. Lesions may extend and become a confluence of plaques. There may be partial central clearing, giving rise to ring like lesions referred to as annular psoriasis, typically associated with lesion resolution and a good prognosis.
Eruptive psoriasis (guttate) is associated more with young adults and is characterized by papules 0.5-1.5 cm in diameter over the upper trunk and proximal extremities. Streptococcal throat infection or other upper airway infection commonly precedes or coexists with a flare of this type of psoriasis. Children usually clear within months while adults may have a more chronic course.
Inverse psoriasis also presents in a different pattern, and is associated with skin folds, including the axilla, neck, and genital area. Scaling in this type of psoriasis is usually minimal or not present at all. The lesions are of a glossy erythema that is well demarcated, and sweating is impaired over the effected skin. Pustulat psoriasis is another variant.
Psoriasis vulgaris is seen in approximately 90 percent of psoriasis patients. Red, scaly plaques are located in extensor areas of the extremities, especially the elbows and knees. Lesions may extend and become a confluence of plaques. There may be partial central clearing, giving rise to ring like lesions referred to as annular psoriasis, typically associated with lesion resolution and a good prognosis.
Eruptive psoriasis (guttate) is associated more with young adults and is characterized by papules 0.5-1.5 cm in diameter over the upper trunk and proximal extremities. Streptococcal throat infection or other upper airway infection commonly precedes or coexists with a flare of this type of psoriasis. Children usually clear within months while adults may have a more chronic course.
Inverse psoriasis also presents in a different pattern, and is associated with skin folds, including the axilla, neck, and genital area. Scaling in this type of psoriasis is usually minimal or not present at all. The lesions are of a glossy erythema that is well demarcated, and sweating is impaired over the effected skin. Pustulat psoriasis is another variant.
|
 Inverse Psoriasis |

Molluscum
Umbilicated Papules of Molluscum
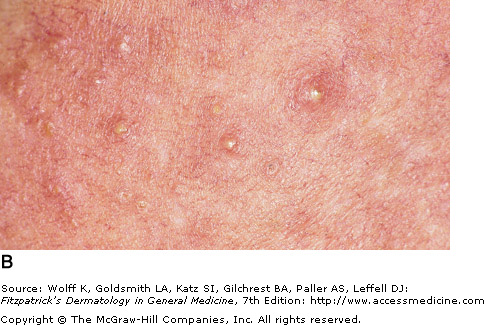
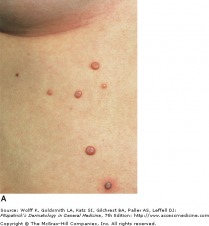
Molluscum contagiosum is a benign viral infection that typically affects young children. In children, the disease is usually self-limiting, but can have a long course, from months to years. The disease is more concerning in the immunocompromised patient.
The lesions present as skin colored, or pearly pink papules with a dome shape that can reach up to 3 cm in diameter. In the middle of the papule, there is a depression, or umbilication, in which a white substance may be seen. The number and extent of lesions can vary, and in immunocompromised patients, lesions are greater in number and in size. In immunocompetent patients, the papules may resolve spontaneously. If persistent or in cosmetically concerning areas, many therapies are available, including liquid nitrogen, cantharidin, and Aldara. For HIV/AIDS patients treatment initially consists of restoring immunity through anti-retroviral therapy; molluscum become more problematic with CD4 counts below 250.
The lesions present as skin colored, or pearly pink papules with a dome shape that can reach up to 3 cm in diameter. In the middle of the papule, there is a depression, or umbilication, in which a white substance may be seen. The number and extent of lesions can vary, and in immunocompromised patients, lesions are greater in number and in size. In immunocompetent patients, the papules may resolve spontaneously. If persistent or in cosmetically concerning areas, many therapies are available, including liquid nitrogen, cantharidin, and Aldara. For HIV/AIDS patients treatment initially consists of restoring immunity through anti-retroviral therapy; molluscum become more problematic with CD4 counts below 250.
Herpes Simplex
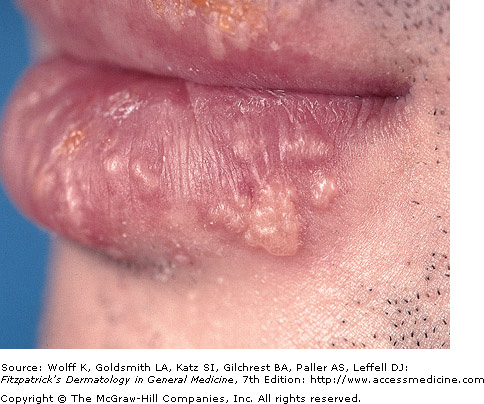
Recurrent HSV-1
Herpes simplex viruses are extremely common DNA viruses. HSV-1 is spread primarily through direct contact with contaminated saliva or secretions, while HSV-2 is spread primarily by sexual contact. The virus replicates at the site of infection, then travels to the dorsal root ganglia, and become latent. The virus may reactivate spontaneously, or in response to a trigger, such as UV light or immunosuppression.
Patients with HSV infection present with a highly variable clinical findings. Lesions in primary infections are initially painful vesicles on an erythematous base. They then progress to pustules and/or ulcerations. It is common to see multiple scattered vesicles, most commonly around the mouth and lips in HSV-1. Lesions will typically crust over and resolve within 2-6 weeks. Lesions occurring after the initial infection are typically less severe and fewer in number. It is not necessary for a person to have a known primary outbreak in order for them to have a latent HSV infection, as asymptomatic infection is common.
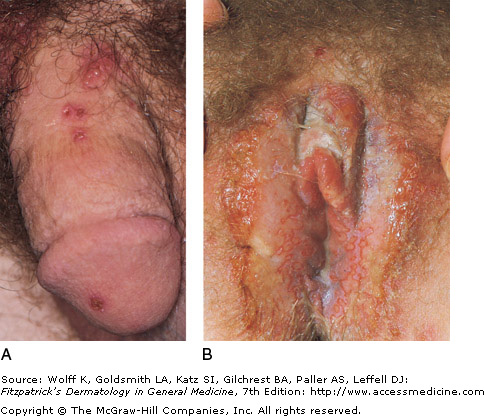
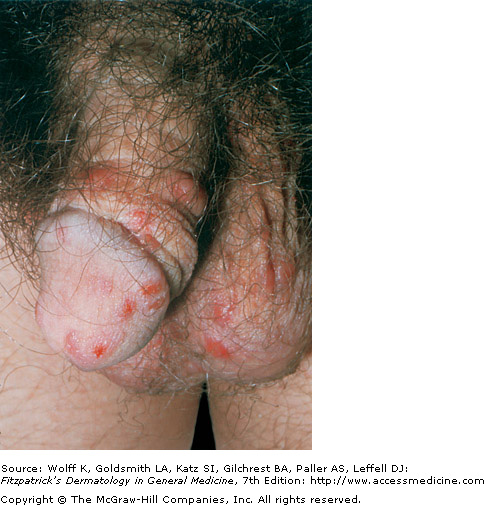
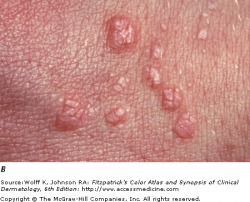
Genital herpes (HSV-2) produces very painful inflammation of the genitalia, and is the most prevalent sexually transmitted infection worldwide. Systemic complications are more common in women, and can include lesions beyond the genitalia, urinary retention, and aseptic meningitis. Primary infection may be distinguished from a recurrent infection with more extensive involvement, lymphadenopathy, and fever. Recurrent infections are typically less severe, and involve three to five vesicles on the genitalia, with resolution in one week.
Patients with HSV infection present with a highly variable clinical findings. Lesions in primary infections are initially painful vesicles on an erythematous base. They then progress to pustules and/or ulcerations. It is common to see multiple scattered vesicles, most commonly around the mouth and lips in HSV-1. Lesions will typically crust over and resolve within 2-6 weeks. Lesions occurring after the initial infection are typically less severe and fewer in number. It is not necessary for a person to have a known primary outbreak in order for them to have a latent HSV infection, as asymptomatic infection is common.
Genital herpes (HSV-2) produces very painful inflammation of the genitalia, and is the most prevalent sexually transmitted infection worldwide. Systemic complications are more common in women, and can include lesions beyond the genitalia, urinary retention, and aseptic meningitis. Primary infection may be distinguished from a recurrent infection with more extensive involvement, lymphadenopathy, and fever. Recurrent infections are typically less severe, and involve three to five vesicles on the genitalia, with resolution in one week.
|
 Recurrent genital herpes infection on penis |

Herpes Zoster

Herpes zoster (shingles) may occur anytime after varicella infection, but is most common after age 50. It can begin with sensitivity, tenderness, pruritis, and/or pain. If intense enough, the pain can even be misdiagnosed as a myocardial infarction or appendicitis. In most cases, a painful eruption of vesicles on an erythematous base develops within a sensory dermatome. The most common site of involvement is the trunk, and in some patients the face or extremities may be involved. In children, herpes zoster usually resolves without sequelae. With increasing age or immunocompromised status, complications become more severe, and can include herpetic neuralgia, secondary bacterial infection, scarring, ophthalmic complications, pneumonitis, motor paralysis, and hepatitis. Acyclovir can shorten the duration and severity of this illness, if administered within 24-72 hours after the onset of skin symptoms.
Impetigo

Common and very contagious, impetigo is a superficial skin infection typically seen in children. Staphylococcus aureus is known to cause all cases of bullous impetigo, and most cases of non-bullous impetigo. The remaining cases of non-bullous impetigo are caused by Streptococcus pyogenes. It is acquired by person to person contact, and adults will most commonly become infected through contact with children.
Non-bullous impetigo accounts for 70 percent of cases, and begins as a 2-4mm erythematous macule. This macule then evolves into a vesicle or pustule. A characteristic superficial erosion with a honey-colored yellow crust is the final stage. Bullous impetigo begins as vesicles which enlarge to transparent bullae up to 5cm in diameter. They are superficial and easily rupture, leaving a shiny varnish erosion behind. There is no thick crust associated with bullous impetigo.
Non-bullous impetigo accounts for 70 percent of cases, and begins as a 2-4mm erythematous macule. This macule then evolves into a vesicle or pustule. A characteristic superficial erosion with a honey-colored yellow crust is the final stage. Bullous impetigo begins as vesicles which enlarge to transparent bullae up to 5cm in diameter. They are superficial and easily rupture, leaving a shiny varnish erosion behind. There is no thick crust associated with bullous impetigo.
Cellulitis

Cellulitis with blistering and crusting
Cellulitis is an infection of the deep dermis and subcutaneous tissue. The most common organisms to cause such infections are S. aureus and S. pyogenes. Bacteria gain access to the dermis by an external or blood-borne route. Many conditions predispose a patient, including alcoholism, diabetes mellitus, malignancy, IV drug use, and peripheral vascular disease.
Often preceded by systemic symptoms of fever, chills, and malaise, affected skin areas present with erythema, tenderness, and pain. The border between effected skin and normal skin is not well defined. In severe infections, vesicles, bullae, and necrotic tissue may be present. Regional lymphadenopathy may occur with cellulitis on an extremity, and recurrent infections may damage the lymphatic tissue. Antimicrobial treatment is targeted towards S. pyogenes and S. aureus, using a full course of an antibiotic with good gram-positive coverage.
Often preceded by systemic symptoms of fever, chills, and malaise, affected skin areas present with erythema, tenderness, and pain. The border between effected skin and normal skin is not well defined. In severe infections, vesicles, bullae, and necrotic tissue may be present. Regional lymphadenopathy may occur with cellulitis on an extremity, and recurrent infections may damage the lymphatic tissue. Antimicrobial treatment is targeted towards S. pyogenes and S. aureus, using a full course of an antibiotic with good gram-positive coverage.
Scabies

Scabies of the interdigital space
Scabies is a superficial epidermal human infestation caused by the mite Sarcoptes scabiei. After an initial incubation period of 6-8 weeks, patients note a diffuse, intense pruritic eruption. The itch is severe as is usually worse at night.
Lesions are red, scaly, and sometimes crusted papules and nodules. The webbed areas of the fingers and toes, wrists, palms, and skin fold areas are preferred sites. Thread-like burrows can be visualized. Often 1-10 mm in length, these burrows result from the travelling of the mite in the stratum corneum. Scrapings from the burrows can be examined under the microscope to provide a definitive diagnosis. Treatment with topical scabicides is often effective, however the itch may persist for up to a month after the completion of proper therapy. Tiamcinolone Cream or ointment, 0.025-0.1, can help to decrease the pruritus.
Lesions are red, scaly, and sometimes crusted papules and nodules. The webbed areas of the fingers and toes, wrists, palms, and skin fold areas are preferred sites. Thread-like burrows can be visualized. Often 1-10 mm in length, these burrows result from the travelling of the mite in the stratum corneum. Scrapings from the burrows can be examined under the microscope to provide a definitive diagnosis. Treatment with topical scabicides is often effective, however the itch may persist for up to a month after the completion of proper therapy. Tiamcinolone Cream or ointment, 0.025-0.1, can help to decrease the pruritus.
|
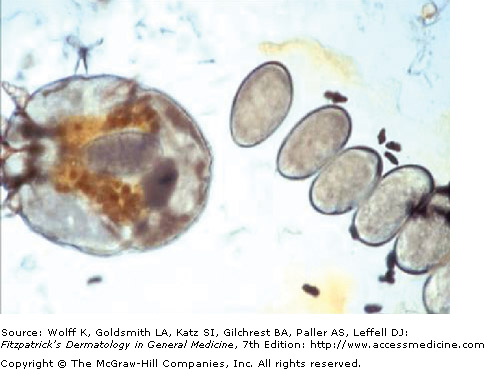 Scabies mite, eggs, and feces on mineral oil prep |

Urticaria
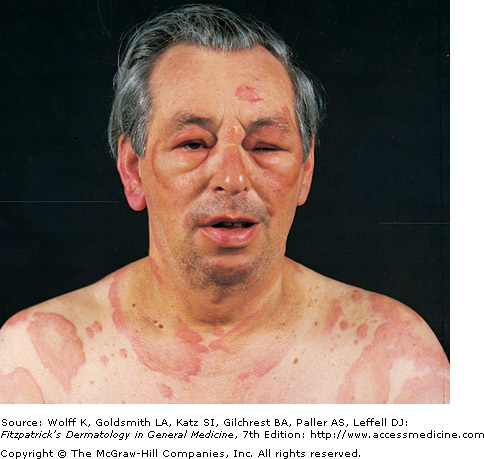
Urticaria with Angioedema around eyes
Urticaria (hives) is a skin lesion consisting of a wheal-and-flare reaction. Intracutaneous edema (wheal) is surrounded by erythema and is often pruritic. Essentially, this is a red, raised, circumscribed area of edema that is accompanied by itching. The wheals come in various sizes, from a millimeter to 8 cm, blanch upon pressure, and may have a central pallor as dilated blood vessels are compressed. These wheals are superficial and well defined. Urticaria lesions appear suddenly and while most clear bt 24 hours, they rarely last longer than 48 hours. They may continue to recur with exposure to the causative factor.
Angioedema can by caused by the same mechanisms that cause urticaria, however swelling is the main manifestation and the process occurs in the deep dermis and subcutaneous tissue.
Acute urticaria and angioedema is caused by a variety of sources, including foods, drugs, infections associated with allergic factors (IgE) or metabolic factors. In chronic urticaria, an autoimmune disorder is present in about 45 percent of patients. Twenty percent of the adult population will experience urticaria or angioedema at some point in their lives.
Treatment often consists of avoidance (if the trigger is known) and antihistamines. Oral corticosteroids may be necessary for severe reactions. A true C1 esterase inhibitor deficiency or decreased activity requires other treatment, as anabolic steroids.
Angioedema can by caused by the same mechanisms that cause urticaria, however swelling is the main manifestation and the process occurs in the deep dermis and subcutaneous tissue.
Acute urticaria and angioedema is caused by a variety of sources, including foods, drugs, infections associated with allergic factors (IgE) or metabolic factors. In chronic urticaria, an autoimmune disorder is present in about 45 percent of patients. Twenty percent of the adult population will experience urticaria or angioedema at some point in their lives.
Treatment often consists of avoidance (if the trigger is known) and antihistamines. Oral corticosteroids may be necessary for severe reactions. A true C1 esterase inhibitor deficiency or decreased activity requires other treatment, as anabolic steroids.
 Classic wheals of utricaria |
 Acute urticaria with small and large wheals |
 Actinic Keratoses on scalp |
 Rough hyperkeratosis |
Tinea Versicolor
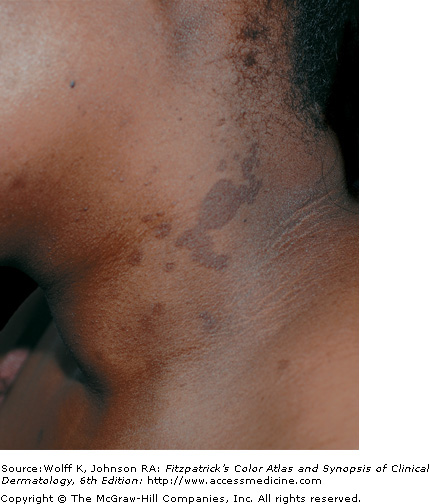
Tinea Versicolor - hyperpigmented
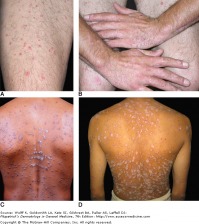
Caused by the fungus Malassezia furfur, tinea versicolor (pityriasis versicolor) presents with many well-demarcated oval patches or thin plaques. These lesions often group together and become confluent and extensive over the body. The most common areas affected are the upper trunk and shoulders. The most common colors are tan (hypopigmented) and brown (hyperpigmented).
-Untanned skin: lesions are light brown -Tanned skin: lesions are hypopigmented -Dark or olive toned skinned persons: lesions are dark brown macules, brown of varying intensities and hues, or off-white macules. -Some lesions are pink
Tinea versicolor is not associated with any serious symptoms, and the main patient concern is cosmetic appearance.
Tinea versicolor is not associated with any serious symptoms, and the main patient concern is cosmetic appearance.
 Tinea Versicolor - hyperpigmented |
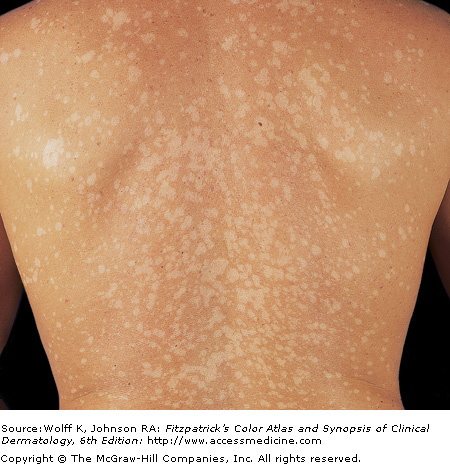 TInea Versicolor - hypopigmented |
Tinea

Tinea Corporis
Dermatophytoses are fungal infections caused by fungi from the genera Microsporum, Trichophyton, and Epidermophyton. These "dermatophytes" are unique because they have the ability to invade and colonize keratinized tissue, such as hair, skin, and nails. They produce enzymes called keratinases that break down keratin tissue, allowing for their invasion. Many host factors are involved in limiting the spread of dermatophyte infection, including the patient's genetic predisposition, immune status, and other underlying diseases.
Tinea corporis: This dermatophyte infection invovles the trunk and extremities, and is generally limited to the stratum corneum. The most common cause is the organism Trichophyton rubrum. Risk factors for this infection include a past history of tinea capitis or tinea pedis, exposure to gymnasiums, locker rooms, and dormitory style housing. Infection spreads in a centrifugal manner from the point of infection with central clearing, leading to annular lesions of different sizes. Many lesions are scaly, and pustules are contained within the active border. The symptoms associated with tinea corporis are burning and pruritis (itching).
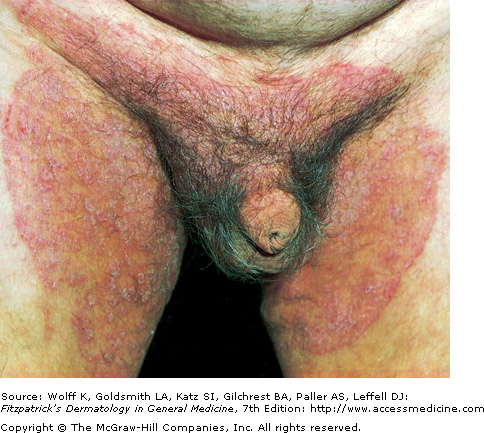
Tinea cruris: A dermatophyte infection of the inguinal region, especially the upper thighs, this condition is more common in men and in obese patients. Classic lesions are well demarcated with a raised, erythematous, scaly advancing border, which may contain pustules or vesicles. The scrotum is typically spared in these infections, and if the scrotum is involved, one should consider candidiasis.
Tinea capitis: This infection is common in the scalp of children, and does not occur frequently in adults. It has a wide range of presentations, from a non-inflammatory scaling to a severe pustular eruption with hair loss. There are many other conditions that caused scalp scaling and hair loss, however fungal infections should be included on the differential. This disease is contagious, and family members should be screened for tinea capitis.
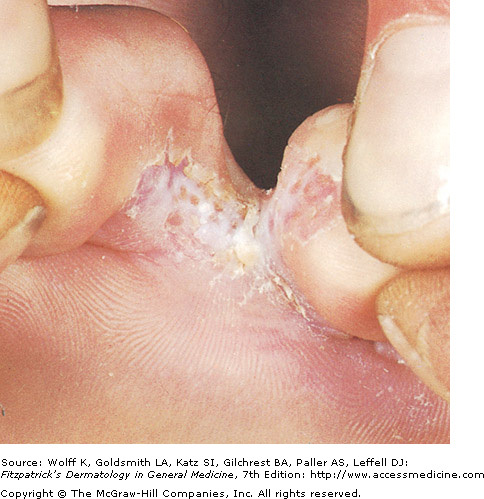
Tinea pedis: A dermatophyte infection of the soles of the feet and interdigital spaces, tinea pedis is a common condition that is thought to be associated with shoes or boots that allow for increased heat and moisture and with walking barefoot in gyms, locker rooms, and public pools. There are four major types of tinea pedis: moccasin, interdigital, inflammatory, and ulcerative. The most common type, interdigital, is associated with erythema, scaling, fissures, and maceration in the web spaces. Itching is common, and the infection can extend to the sole of the foot.
Tinea corporis: This dermatophyte infection invovles the trunk and extremities, and is generally limited to the stratum corneum. The most common cause is the organism Trichophyton rubrum. Risk factors for this infection include a past history of tinea capitis or tinea pedis, exposure to gymnasiums, locker rooms, and dormitory style housing. Infection spreads in a centrifugal manner from the point of infection with central clearing, leading to annular lesions of different sizes. Many lesions are scaly, and pustules are contained within the active border. The symptoms associated with tinea corporis are burning and pruritis (itching).
Tinea cruris: A dermatophyte infection of the inguinal region, especially the upper thighs, this condition is more common in men and in obese patients. Classic lesions are well demarcated with a raised, erythematous, scaly advancing border, which may contain pustules or vesicles. The scrotum is typically spared in these infections, and if the scrotum is involved, one should consider candidiasis.
Tinea capitis: This infection is common in the scalp of children, and does not occur frequently in adults. It has a wide range of presentations, from a non-inflammatory scaling to a severe pustular eruption with hair loss. There are many other conditions that caused scalp scaling and hair loss, however fungal infections should be included on the differential. This disease is contagious, and family members should be screened for tinea capitis.
Tinea pedis: A dermatophyte infection of the soles of the feet and interdigital spaces, tinea pedis is a common condition that is thought to be associated with shoes or boots that allow for increased heat and moisture and with walking barefoot in gyms, locker rooms, and public pools. There are four major types of tinea pedis: moccasin, interdigital, inflammatory, and ulcerative. The most common type, interdigital, is associated with erythema, scaling, fissures, and maceration in the web spaces. Itching is common, and the infection can extend to the sole of the foot.
|
|


Lichen Planus

Lichen Planus on wrist
Lichen planus is an inflammatory disorder of the skin, mucous membranes, hair, and nails. It is characterized with distinct symmetric, group, violet colored, flat-topped, polygonal papules. The "Four Ps" of purple, polygonal, pruritic, papule, are used to remember the symptoms of lichen planus. The distribution can be widespread, but favors the flexural areas of the arms and legs. Lesions are often symmetrical and bilateral over the extremities. The oral and genital areas may also be involved, and the face is generally spared.
The classic lesion, as mentioned in the mnemonic, is an erythematous/violaceous, flat-topped, polygonal papule. There may be a slight central umbilication of the papule, and the lesions tend to be grouped together, with a tendency to coalesce. Lichen planus is often pruritic, but can be asymptomatic in some individuals. Treatments include topical glucocorticoids, and if necessary, systemic oral prednisone (tapered course) and cyclosporine.
The classic lesion, as mentioned in the mnemonic, is an erythematous/violaceous, flat-topped, polygonal papule. There may be a slight central umbilication of the papule, and the lesions tend to be grouped together, with a tendency to coalesce. Lichen planus is often pruritic, but can be asymptomatic in some individuals. Treatments include topical glucocorticoids, and if necessary, systemic oral prednisone (tapered course) and cyclosporine.
 Flat top, polygonal papules of Lichen Planus |
|

Verrucae (warts)

Common flat-topped warts
Verrucae, commonly known as warts, are benign proliferations of skin caused by papillomavirus infection. Rather than acute signs of infection, the viruses produce a slow, focal expansion of epithelial cells with surface hyperkeratosis. Subsets of HPV infection are associated with cerival, penile, anal, and epithelial malignancies.
Patients typically present with a history of a slowly expanding, scaly lesion. Over the course of several weeks to months, new lesions in the same location is suggestive of local spread of HPV infection. Common warts (verruca vulgaris) are scaly, rough, shiny papules that may erupt on any cutaneous surface. Under magnification, some warts show brown or red spots indicating thrombosed capillaries. Flat warts are elevated, flat topped papules measuring 1-4 mm in diameter, and occur most frequently on the face, hands, and lower legs. Plantar and palmar warts may be painful with pressure, even to the point of impeding walking. They are thick, hyperkeratotic papules, and may coalesce into mosaic warts, forming large plaques.
Anogenital warts are epidermal and dermal papules or nodules on the genitalia, perineum, or crural folds. In the moist environment, they may form large, cauliflower-like masses. Warts may even extend inward into the vaginal canal, urethra, and rectum.
The treatment of warts depends on the patient's level of discomfort (either physical or cosmetic) and their desire for treatment. Most treatments focus on destroying the infected cells, and recurrences may occur. Cryotherapy is a common and effective treatment for most warts, in which liquid nitrogen is applied to the skin to achieve a halo of ice around the lesion. Warts may also be removed through surgical methods, and topical therapies are also available.
Patients typically present with a history of a slowly expanding, scaly lesion. Over the course of several weeks to months, new lesions in the same location is suggestive of local spread of HPV infection. Common warts (verruca vulgaris) are scaly, rough, shiny papules that may erupt on any cutaneous surface. Under magnification, some warts show brown or red spots indicating thrombosed capillaries. Flat warts are elevated, flat topped papules measuring 1-4 mm in diameter, and occur most frequently on the face, hands, and lower legs. Plantar and palmar warts may be painful with pressure, even to the point of impeding walking. They are thick, hyperkeratotic papules, and may coalesce into mosaic warts, forming large plaques.
Anogenital warts are epidermal and dermal papules or nodules on the genitalia, perineum, or crural folds. In the moist environment, they may form large, cauliflower-like masses. Warts may even extend inward into the vaginal canal, urethra, and rectum.
The treatment of warts depends on the patient's level of discomfort (either physical or cosmetic) and their desire for treatment. Most treatments focus on destroying the infected cells, and recurrences may occur. Cryotherapy is a common and effective treatment for most warts, in which liquid nitrogen is applied to the skin to achieve a halo of ice around the lesion. Warts may also be removed through surgical methods, and topical therapies are also available.
|
 Multiple genital warts |

Basal Cell Carcinoma

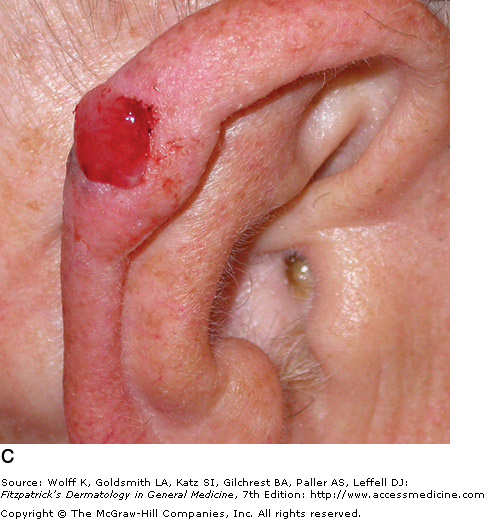
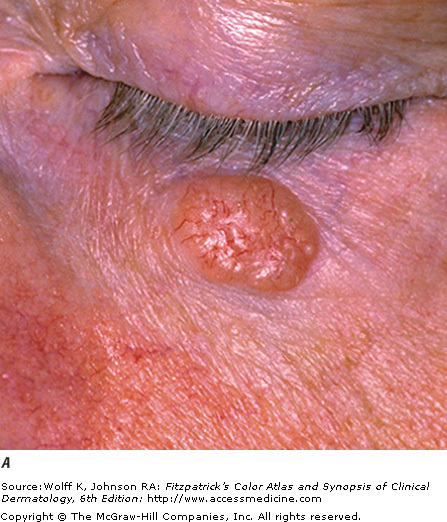
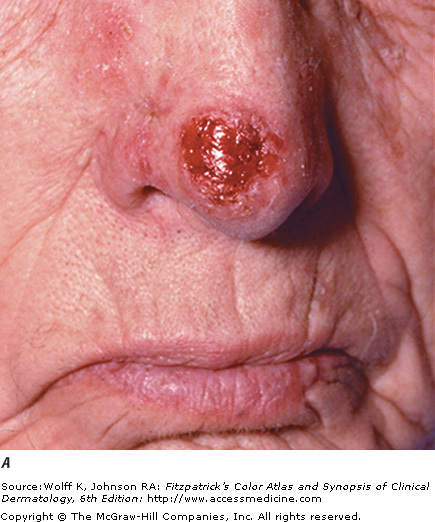
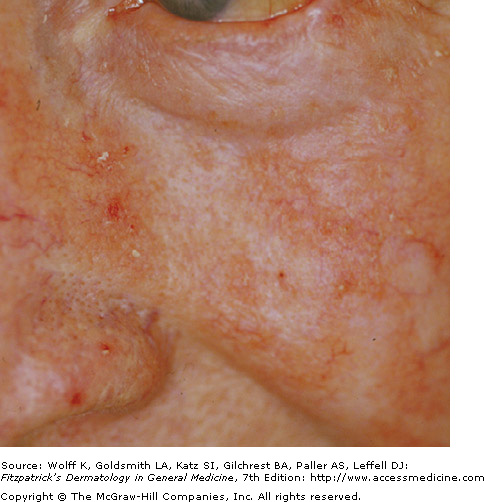
Noduler BCC on nose
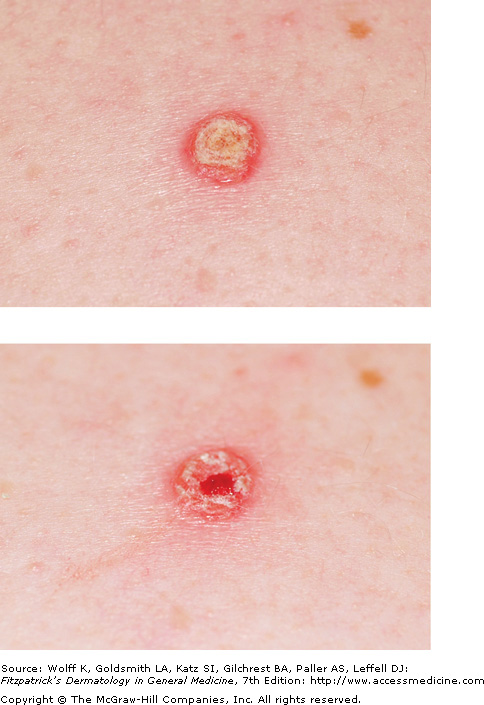
Basal cell carcinoma (BCC) is a malignant neoplasm of nonkeratinizing cells from the basal layer of the epidermis. While basal cell carcinomas will spread locally and destroy surrounding tissue, metastasis is extraordinarily rare. BCC is the most common cancer in humans, and is caused by ultraviolet light exposure (particularly the UVB spectrum) inducing mutations in tumor suppressor genes. BCC is also associated with a mutation in the PTCH gene.
Nodular basal cell carcinoma is the most common sub-type, and occurs commonly on sun-exposed areas of the head and neck. The lesion is a translucent skin colored to red papule or nodule, usually with telangiectasias and a rolled border. Portions of a nodular BCC may have erosions or spots of melanin pigmentation.
Pigmented basal cell carinoma are brown, blue, or black with a smooth glistening surface. They are a variant of nodular BCC, but have increased melanization. Papules are translucent, and may be eroded. Upon palpation, pigmented BCCs are hard and firm. Pigmented BCC may look deceptively similar to malignant melanoma, a deadly form of skin cancer.
Superficial basal cell carcinoma commonly occurs on the trunk as a well demarcated erythematous patch. It may appear similar to eczema, and any isolated patch of eczema not responding to treatment should raised suspicion of a potential superficial BCC. It is the only form of BCC that exhibits significant scaling, and telangiectasias may be seen upon magnification.
Morpheaform (sclerosing) basal cell carcinoma appears as a small superficial scar, skin colored (with peppered pigmentation) and ill-defined. These forms of BCC grow deep and wide, often requiring a large area of surgical excision. The presence of "scar tissue" at a site where there is no history of trauma or surgery should raise suspicion for morpheaform BCC. Morpheaform BBC has the ability to progress to nodular or ulcerating BCC.
Ulcerating basal cell carcinoma ulcer with a rolled border, and is often covered by a crust. Lesions are translucent, pearly, telangiectatic, smooth, and firm.
Lesions raising suspicion for BCC should be referred to a dermatologist for examination, biopsy, and possible excision. A variety of surgical techniques, including Mohs surgery, are available for the treatment of basal cell carcinoma.
Nodular basal cell carcinoma is the most common sub-type, and occurs commonly on sun-exposed areas of the head and neck. The lesion is a translucent skin colored to red papule or nodule, usually with telangiectasias and a rolled border. Portions of a nodular BCC may have erosions or spots of melanin pigmentation.
Pigmented basal cell carinoma are brown, blue, or black with a smooth glistening surface. They are a variant of nodular BCC, but have increased melanization. Papules are translucent, and may be eroded. Upon palpation, pigmented BCCs are hard and firm. Pigmented BCC may look deceptively similar to malignant melanoma, a deadly form of skin cancer.
Superficial basal cell carcinoma commonly occurs on the trunk as a well demarcated erythematous patch. It may appear similar to eczema, and any isolated patch of eczema not responding to treatment should raised suspicion of a potential superficial BCC. It is the only form of BCC that exhibits significant scaling, and telangiectasias may be seen upon magnification.
Morpheaform (sclerosing) basal cell carcinoma appears as a small superficial scar, skin colored (with peppered pigmentation) and ill-defined. These forms of BCC grow deep and wide, often requiring a large area of surgical excision. The presence of "scar tissue" at a site where there is no history of trauma or surgery should raise suspicion for morpheaform BCC. Morpheaform BBC has the ability to progress to nodular or ulcerating BCC.
Ulcerating basal cell carcinoma ulcer with a rolled border, and is often covered by a crust. Lesions are translucent, pearly, telangiectatic, smooth, and firm.
Lesions raising suspicion for BCC should be referred to a dermatologist for examination, biopsy, and possible excision. A variety of surgical techniques, including Mohs surgery, are available for the treatment of basal cell carcinoma.
|
|

|
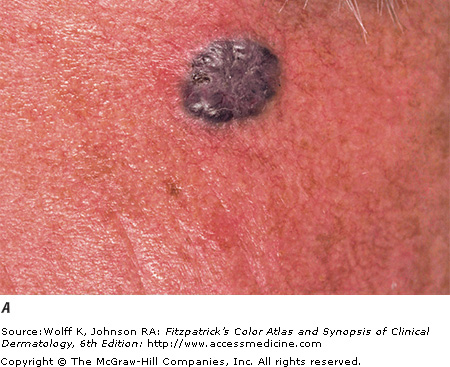 PIgmented BCC |

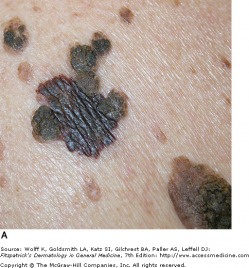
Seborrheic Keratosis

Seborrheic keratosis -lackluster appearance
Seborrheic keratosis is the most common type of benign epidermal tumor. They are a common cause of dermatologist referrals due to their variable appearance, and may appear similar to certain types of skin cancers. SKs initially appear as well-circumscribed patches that are dull, flat, tan, or brown.
As they grow and evolve, they become more papular, appearing as if they were "stuck on." The color of the lesions can range from pale white to black, and differentiating SKs from melanoma can at times be difficult. It is very important to evaluate any lesion that is growing rapidly, symptomatic, or unusual for the particular patient.
As they grow and evolve, they become more papular, appearing as if they were "stuck on." The color of the lesions can range from pale white to black, and differentiating SKs from melanoma can at times be difficult. It is very important to evaluate any lesion that is growing rapidly, symptomatic, or unusual for the particular patient.
 Multiple small seborrheic keratoses |
 Multiple reticulated seborrheic keratoses |
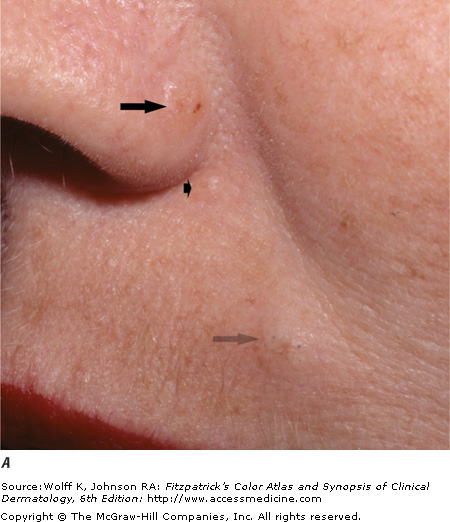
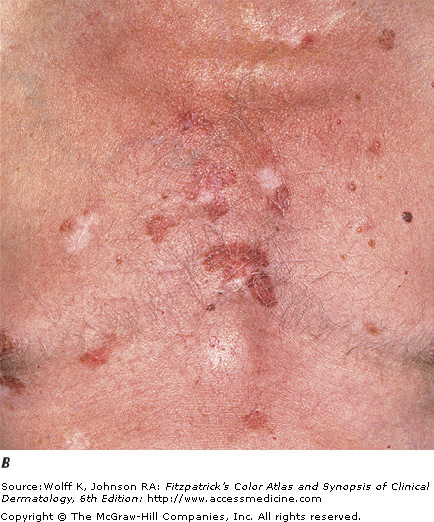
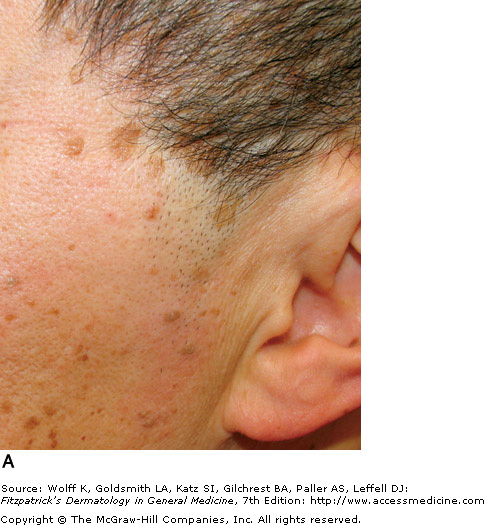
Actinic Keratosis
AKs on sun damaged skin
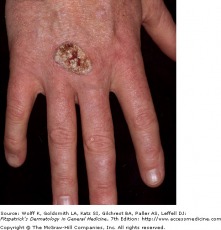
Actinic keratoses (AKs) are cutaneous neoplasms of proliferating keratinocytes which develop after prolonged exposure to UV light. AKs have traditionally been known as precancerous lesions with the potential to develop into squamous cell carcinoma. They are clinically important, not only because they may become squamous cell cancers, but because they are strong predictors of patient risk for developing melanoma and other skin cancers. Individuals with AKs should be closely monitored and screened for the prevention and detection of skin cancers. A full body skin exam is very important, including lower extremities.
Actinic keratosis is the second most common reason for visits to a dermatologist. The typical patient is older, fair-skinned, with light eye color and a history of sun exposure with burning or freckling rather than tanning. Most AKs are found on normally sun-exposed sites such as the neck, head, forearms, and hands.
The erythematous actinic keratosis lesion commonly presents as a erythematous, flat, rough, scaly papule that is 2-6 mm in diameter, yet can reach several centimeters in diameter. Some AKs are more easily felt than seen. They are most often found in areas of sun damaged skin, telangiectases, and sagging skin. Many AKs may be present and confluent, giving the appearance of a rash. Due to the risk of developing squamous cell cancer, most dermatologist advocate for the treatment of AKs. Many different procedural and pharmaceutical treatment options are available.
Actinic keratosis is the second most common reason for visits to a dermatologist. The typical patient is older, fair-skinned, with light eye color and a history of sun exposure with burning or freckling rather than tanning. Most AKs are found on normally sun-exposed sites such as the neck, head, forearms, and hands.
The erythematous actinic keratosis lesion commonly presents as a erythematous, flat, rough, scaly papule that is 2-6 mm in diameter, yet can reach several centimeters in diameter. Some AKs are more easily felt than seen. They are most often found in areas of sun damaged skin, telangiectases, and sagging skin. Many AKs may be present and confluent, giving the appearance of a rash. Due to the risk of developing squamous cell cancer, most dermatologist advocate for the treatment of AKs. Many different procedural and pharmaceutical treatment options are available.
 Yellow-gray scales of an AK |
 Solar keratosis |
Squamous Cell Carcinoma In Situ

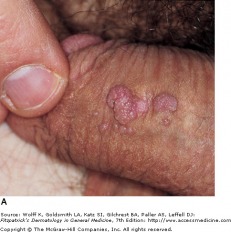
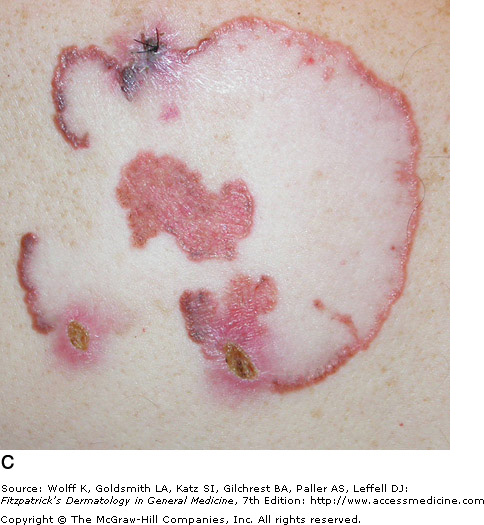
Squamous cell carcinoma in situ presents as a slowly enlarging, pink/erythematous thin plaque with well-demarcated, yet irregular borders with an overlying scale or crust. SCC in situ may look similar to a psoriasis plaque. Lesions commonly occur in sun-exposed areas, and may become several centimeters in diameter. It has been estimated that approximately 3-5 percent of SCC in situ lesions progress to an invasive carcinoma. Surgical, topical, and laser therapies exist for SCC in situ.
Squamous Cell Carcinoma

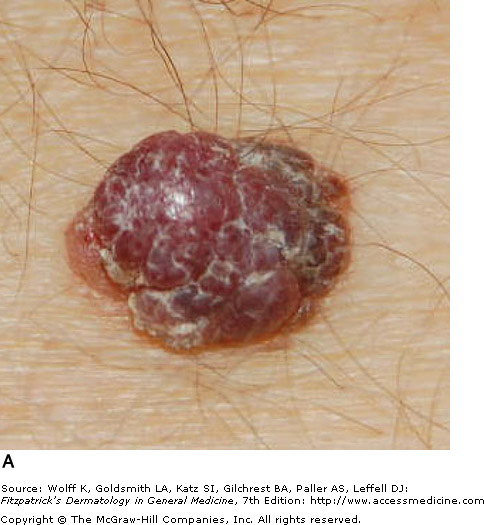
Well differentiated SCC
Squamous cell carcinomas (SCC) are malignant neoplasms arising from keratinocytes above the basal layer of the epidermis. It is thought that most cases of SCC evolve from precursor lesions, such as actinic keratoses or squamous cell carcinoma in situ. SCC encompass a broad clinical spectrum, from easily managed lesions to highly-infiltrative tumors that may result in death.
In slowly evolving cases, any isolated keratotic or eroded papule/plaque that persists for over a month should be considered cancerous until proven otherwise. SCC is asymptomatic when it is slowly evolving. In rapidly evolving cases, SCC may present with symptoms of pain or tenderness.
Well differentiated SCC almost always shows keratinization of the tumor or surface of the tumor, and are firm upon palpation. Poorly differentiated SCC do not exhibit keratinization and are fleshy or granulomatous in appearance. They are soft upon palpation.
Differentiated SCC usually present with an isolated lesions, however they can be multiple. Distribution is often in sun-exposed areas, and the indurate papule, plaque, or macule may be erythematous, yellow, or skin colored. Undifferentiated SCC lesions are fleshy nodules and erosive papules that bleed easily and are often crusted. Lesions are also soft, and may appear polygonal, irregular, or cauliflower-like in shape.
In slowly evolving cases, any isolated keratotic or eroded papule/plaque that persists for over a month should be considered cancerous until proven otherwise. SCC is asymptomatic when it is slowly evolving. In rapidly evolving cases, SCC may present with symptoms of pain or tenderness.
Well differentiated SCC almost always shows keratinization of the tumor or surface of the tumor, and are firm upon palpation. Poorly differentiated SCC do not exhibit keratinization and are fleshy or granulomatous in appearance. They are soft upon palpation.
Differentiated SCC usually present with an isolated lesions, however they can be multiple. Distribution is often in sun-exposed areas, and the indurate papule, plaque, or macule may be erythematous, yellow, or skin colored. Undifferentiated SCC lesions are fleshy nodules and erosive papules that bleed easily and are often crusted. Lesions are also soft, and may appear polygonal, irregular, or cauliflower-like in shape.
|
|




Malignant Melanoma
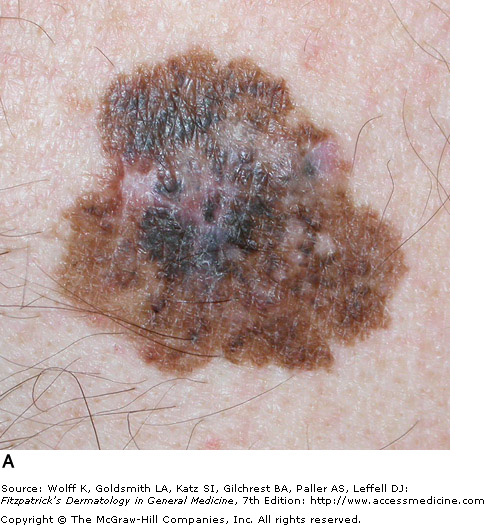
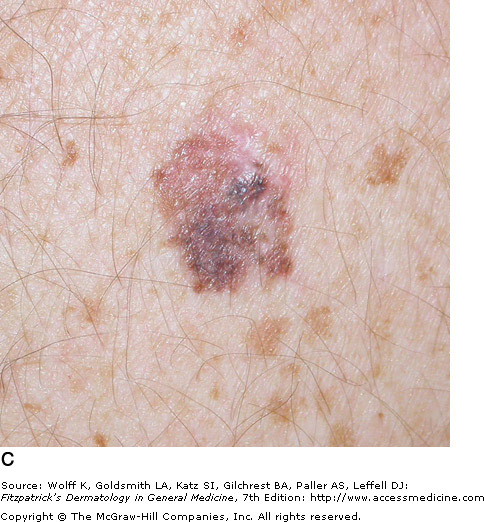
Classic superficial spreading melanoma
The incidence of melanoma has increased dramatically within the past decades. Lifetime risk of invasive melanoma for a person born in 1935 was 1 in 1500, and lifetime risk for a person born in 2006 is now estimated at 1 in 62. Melanoma is responsible for the majority of fatalities associated with skin cancer, with approximately 8000 patient deaths in 2006. One of the particularly tragic aspects of melanoma is a relatively young age of diagnosis. The mean age for diagnosis is 52 years, which is 10-15 years younger than other more common cancers. Melanoma follows a highly-variable course, and is often curable if treated early, but is potentially fatal if diagnosed and treated late.
For melanoma recognition, the ABCDE checklist can be a helpful reminder:
-A: asymmetry
-B: irregular borders
-C: color
-D: diameter > 6 mm is common
-E: evolving over time
There are many known risk factors for melanoma, some of which are a history of sunburns or heavy sun exposure. Skin type, such as fair complexion, red hair, blue or green eyes, are also associated with a higher risk of melanoma. Other factors are a family history of melanoma and the p16 genetic mutation.
Superficial spreading melanoma is the most common subtype, making up approximately 70 percent of cutaneous melanomas. It is diagnosed most often during the fourth of fifth decade of life, and often found on the upper back of men, and lower extremity of women. While lesions on intermittently sun-exposed areas are common, it is important to note that melanomas can occur anywhere on the body, so a full skin check is necessary for detection. The classic appearance has the ABCD signs, but the appearance can be subtle and variable. Superficial spreading melanoma can be associated with pre-existing nevi (dark skin spots) that change over long periods of time. As a result, the melanoma may be mistaken for an atypical nevus or seborrheic keratosis (see above).
Nodular melanoma is the second most common subtype. It is known for rapid evolution, occurring over weeks to months. It is more common for nodular melanoma to arise as a new lesion, rather than from a pre-existing nevus, and appears as a dark blue/black raised lesion. Early nodular melanomas typically lack asymmetry, but have irregular borders and a diameter larger than 6 mm. Nodular melanomas that are not pigmented may be misdiagnosed as basal cell carcinoma or hemangioma, while pigmented lesions may be confused for pigmented basal cell carcinoma or blue nevi.
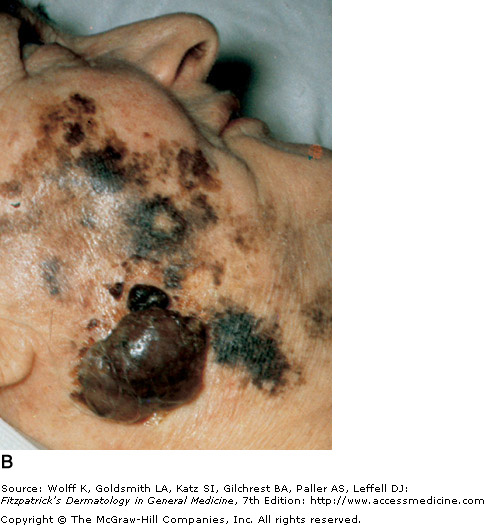
Lentigo maligna (LM) is a subtype of melanoma in situ with prolonged radial growth, which may then progress to lentigo maligna melanoma (LMM). These conditions are more common in the seventh and eighth decades of life, and while the risk of developing LMM is relatively low, it is potentially lethal. LM and LMM have higher rates of recurrence and are more difficult to completely remove. The most common locations are chronically sun exposed areas (head and neck). LM is a flat, slowly enlarging macule that may appear freckle-like with an irregular shape. LMM is frequently larger and often has a nodular form.
Acral lentiginous melanoma accounts for a very small percent of melanomas in Caucasians, but represents a large portion of melanoma in black patients (72%) and Asians (46%). Common sites for acral lentiginous melanoma are the sole
For melanoma recognition, the ABCDE checklist can be a helpful reminder:
-A: asymmetry
-B: irregular borders
-C: color
-D: diameter > 6 mm is common
-E: evolving over time
There are many known risk factors for melanoma, some of which are a history of sunburns or heavy sun exposure. Skin type, such as fair complexion, red hair, blue or green eyes, are also associated with a higher risk of melanoma. Other factors are a family history of melanoma and the p16 genetic mutation.
Superficial spreading melanoma is the most common subtype, making up approximately 70 percent of cutaneous melanomas. It is diagnosed most often during the fourth of fifth decade of life, and often found on the upper back of men, and lower extremity of women. While lesions on intermittently sun-exposed areas are common, it is important to note that melanomas can occur anywhere on the body, so a full skin check is necessary for detection. The classic appearance has the ABCD signs, but the appearance can be subtle and variable. Superficial spreading melanoma can be associated with pre-existing nevi (dark skin spots) that change over long periods of time. As a result, the melanoma may be mistaken for an atypical nevus or seborrheic keratosis (see above).
Nodular melanoma is the second most common subtype. It is known for rapid evolution, occurring over weeks to months. It is more common for nodular melanoma to arise as a new lesion, rather than from a pre-existing nevus, and appears as a dark blue/black raised lesion. Early nodular melanomas typically lack asymmetry, but have irregular borders and a diameter larger than 6 mm. Nodular melanomas that are not pigmented may be misdiagnosed as basal cell carcinoma or hemangioma, while pigmented lesions may be confused for pigmented basal cell carcinoma or blue nevi.
Lentigo maligna (LM) is a subtype of melanoma in situ with prolonged radial growth, which may then progress to lentigo maligna melanoma (LMM). These conditions are more common in the seventh and eighth decades of life, and while the risk of developing LMM is relatively low, it is potentially lethal. LM and LMM have higher rates of recurrence and are more difficult to completely remove. The most common locations are chronically sun exposed areas (head and neck). LM is a flat, slowly enlarging macule that may appear freckle-like with an irregular shape. LMM is frequently larger and often has a nodular form.
Acral lentiginous melanoma accounts for a very small percent of melanomas in Caucasians, but represents a large portion of melanoma in black patients (72%) and Asians (46%). Common sites for acral lentiginous melanoma are the sole
|
|
|
|