Bacterial skin infections are responsible for almost 20 percent of outpatient dermatology visits. Furthermore, the skin can be an excellent indicator of systemic conditions. Bacterial skin infections fall within four general categories: primary skin infection, secondary infection of a primary skin disease, skin lesions due to primary infection of another organ system, or a reactive skin condition from a bacterial infection. In this module, we will primarily concern ourselves with the cutaneous manifestations of systemic diseases and diseases of other organ systems, as well as their reactive conditions.
Staphylococcal and Streptococcal Infections
Impetigo

Non-bullous Impetigo
Common and very contagious, impetigo is a superficial skin infection typically seen in children. Staphylococcus aureus is known to cause all cases of bullous impetigo, most being phage II, type 71. It also most cases of non-bullous impetigo. The remaining cases of non-bullous impetigo are caused by Streptococcus pyogenes. It is acquired by person to person contact, and adults will most commonly become infected through contact with children.
Non-bullous impetigo accounts for 70 percent of cases, and begins as a 2-4mm erythematous macule. This macule then evolves into a vesicle or pustule. A characteristic superficial erosion with a honey-colored yellow crust is the final stage. Bullous impetigo begins as vesicles which enlarge to transparent bullae up to 5cm in diameter. They are superficial and easily rupture, leaving a shiny varnish erosion behind. There is no thick crust associated with bullous impetigo.
Non-bullous impetigo accounts for 70 percent of cases, and begins as a 2-4mm erythematous macule. This macule then evolves into a vesicle or pustule. A characteristic superficial erosion with a honey-colored yellow crust is the final stage. Bullous impetigo begins as vesicles which enlarge to transparent bullae up to 5cm in diameter. They are superficial and easily rupture, leaving a shiny varnish erosion behind. There is no thick crust associated with bullous impetigo.
Staphylococcal Scalded Skin Syndrome
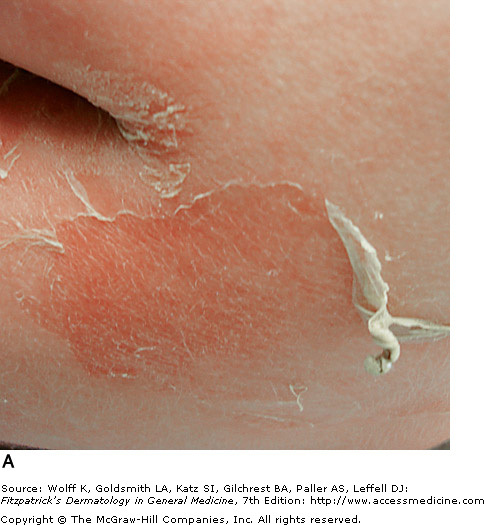
Late Stage SSSS - Fitzpatrick's Dermatology
Staphylococcal scalded skin syndrome is a toxin-mediated manifestation of staphylococcal infection. In SSSS, the epidermis cleaves through the granular layer, leading to flaccid bullae. It typically affects children under the age of six years. Exfoliative toxins ET-A and ET-B affect the granular layer and cause the sterile bullae.
SSSS begins as an erythema, typically limited to the head, but then spreads to the entire body within hours. Skin then develops a wrinkled appearance, and in 1-2 days, bullae are sloughed. This leaves behind areas of moist skin and varnish-like crusts. Scaling and desquamation occur over 3-5 days, and within 10-14 days, the skin heals without scaring.
SSSS begins as an erythema, typically limited to the head, but then spreads to the entire body within hours. Skin then develops a wrinkled appearance, and in 1-2 days, bullae are sloughed. This leaves behind areas of moist skin and varnish-like crusts. Scaling and desquamation occur over 3-5 days, and within 10-14 days, the skin heals without scaring.
Scarlet Fever

Exanthemous Rash with Sandpaper Texture
Scarlet fever is caused by toxins A, B, and C produced by streptococcus pyogenes (group A strep). It commonly affects children age 1-10 years. The toxins produce skin manifestations by delayed-type hypersensitivity reaction, often following tonsillitis or pharyngitis.
A rash typically begins on the neck, chest, and axilla 12-48 hours after the onset of infection symptoms, and spreads across the body. The rash in blanchable and looks like a sunburn with tiny papules. The patient's throat is red and develops an exudate after 3-4 days. The tongue is first white in color with red papillae (white strawberry tongue) and then becomes a beefy red (red strawberry tongue). After 7-10 days desquamation occurs and lasts 2-6 weeks, most affecting the hands and feet.
A rash typically begins on the neck, chest, and axilla 12-48 hours after the onset of infection symptoms, and spreads across the body. The rash in blanchable and looks like a sunburn with tiny papules. The patient's throat is red and develops an exudate after 3-4 days. The tongue is first white in color with red papillae (white strawberry tongue) and then becomes a beefy red (red strawberry tongue). After 7-10 days desquamation occurs and lasts 2-6 weeks, most affecting the hands and feet.
Staphlococcal Toxic Shock Syndrome

Toxic Shock Syndrome - Fitzpatrick's Dermatology
Rapidly progressive and often fatal, STSS is caused by streptococcus pyogenes (Group A Strep) infection. It often presents with fever, shock, soft-tissue infection, and multisystem organ failure. STSS most commonly affects previously healthy people ages 20-50 years old. STSS is believed to be caused by direct tissue invasion and destruction, and cytokine induction by streptococcal pyogenic exotoxins.
Patients with STSS can present with varying skin problems. Fifty percent will show signs of underlying soft tissue infection, such as swelling, tenderness and erythema. Desquamation of the hands and feet occurs in approximately 20 percent of patient. Evidence for a deeper infection may include violaceous vesicles and bullae. These complications could be due to necrotizing fasciitis or myositis.
Patients with STSS can present with varying skin problems. Fifty percent will show signs of underlying soft tissue infection, such as swelling, tenderness and erythema. Desquamation of the hands and feet occurs in approximately 20 percent of patient. Evidence for a deeper infection may include violaceous vesicles and bullae. These complications could be due to necrotizing fasciitis or myositis.
Cellulitis

Recurrent Cellulitis with Lymphedema
Cellulitis is an infectious process of the deep dermis and subcutaneous tissue. The most common causes of cellulitis are S. pyogenes and S. aureus in immunocompetent adults and access usually comes from an abrasion or cut in the skin. It is most often preceded by systemic infection symptoms such as fever, chills, and malaise.
The lesion is ill-defined and does not have palpable borders. In severe cases, vesicles, bullae, pustules, and even necrotic tissue may be present. Regional lymph nodes may be swollen and ascending lymphangitis can occur. Although complications are rare, the lymph vessels can be damaged, leading to recurrent cellulitis.
The lesion is ill-defined and does not have palpable borders. In severe cases, vesicles, bullae, pustules, and even necrotic tissue may be present. Regional lymph nodes may be swollen and ascending lymphangitis can occur. Although complications are rare, the lymph vessels can be damaged, leading to recurrent cellulitis.
Necrotizing Fasciitis

Necrotizing Fasciitis - Schwartz's Surgery
Also terrifyingly known as flesh-eating bacteria syndrome, necrotizing fasciitis is a rapidly progressing necrosis of subcutaneous fat and fascia. This condition can be life threatening without surgical and antibiotic treatment. A subgroup of necrotizing fasciitis caused by group A streptococcus often occurs in young patients who were previously healthy. Infection can occur after a traumatic injury, or without injury at all. Most cases are actually a mixed infection of aerobic and anaerobic bacteria, reflecting organisms that were introduced by trauma or surgical procedures.
The initial site of infection begins as a very tender, erythematous, hot, and swollen area that is non-responsive to antibiotics. The skin initially appears shiny and tense, and rapidly progresses to a red/purple and then to gray-blue with ill-defined patches. All of these changes occur within 36 hours. Necrosis of the fascia and fat produces a fluid that is thin and watery. Cutaneous nerves may be destroyed, causing anesthesia in the region. On palpation, the subcutaneous tissue may feel very hard and firm.
The initial site of infection begins as a very tender, erythematous, hot, and swollen area that is non-responsive to antibiotics. The skin initially appears shiny and tense, and rapidly progresses to a red/purple and then to gray-blue with ill-defined patches. All of these changes occur within 36 hours. Necrosis of the fascia and fat produces a fluid that is thin and watery. Cutaneous nerves may be destroyed, causing anesthesia in the region. On palpation, the subcutaneous tissue may feel very hard and firm.
Myonecrosis (Gas Gangrene)

Gas Gangrene - Atlas of Emergency Medicine
Clostridial myonecrosis is an infection of muscle that is rapidly progressive and potentially lethal. It occurs after trauma or surgery on the bowel or gallbladder or in the elderly population with diabetes mellitus or peripheral vascular disease. Skin changes include dark yellow or bronze discoloration, bullae filled with brown fluid, and patches of necrosis with foul-smelling exudate. The lesion in extremely painful and swollen. Crepitus (popping sound of gas bubbles under the skin) if present is helpful in supporting the diagnosis, but is not required. The patient has other toxic symptoms, including fever, tachycardia, and hypotension.
C. perfringes is the most common culprit, occuring in 80 percent of cultures. Cultures are used to distinguish this condition form necrotizing fasciitis. Treatment, like necrotizing fasciitis, involved surgical debridement and antibiotic therapy.
C. perfringes is the most common culprit, occuring in 80 percent of cultures. Cultures are used to distinguish this condition form necrotizing fasciitis. Treatment, like necrotizing fasciitis, involved surgical debridement and antibiotic therapy.
