Acute and Chronic Meningococcemia - Neisseria meningitidis
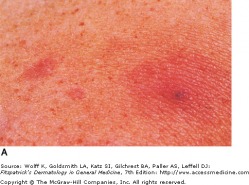
Macular and Papular Lesions on Upper Chest
Meningococcemia is characterized by fever and a petechial eruption. It has two forms, acute and chronic, both caused by the bacteria Neisseria meningitidis, an aerobic gram negative diplococcus. Meningococcal infection primarily affects children 6 months to 1 year old, and young adults living in close quarters.
Of the patients that develop acute meningococcemia, approximately one third to one half will develop a petechial eruption. This can then evolve to ecchymoses and ischemic necrosis. Further complications, such as disseminated intravascular coagulation (DIC) can present with other skin lesions, including large areas of purpura.
Chronic meningococcemia is rare, but involves fever, arthralgias, and a skin eruption that are commonly erythematous macules, papules, and plaques. These skin lesions develop 12-24 hours after the onset of fever.
Of the patients that develop acute meningococcemia, approximately one third to one half will develop a petechial eruption. This can then evolve to ecchymoses and ischemic necrosis. Further complications, such as disseminated intravascular coagulation (DIC) can present with other skin lesions, including large areas of purpura.
Chronic meningococcemia is rare, but involves fever, arthralgias, and a skin eruption that are commonly erythematous macules, papules, and plaques. These skin lesions develop 12-24 hours after the onset of fever.
Bartonellosis (Oroya Fever)

Verruga Peruana of Bartonellosis - Fitzpatrick's
Caused by the pleomorphic gram-negative bacteria Bartonella bacilliformis, Bartonellosis is a biphasic illness. The initial phase consists of fever and hemolytic anemia, and is then followed by an eruption of skin lesions call verruga peruana, or Peruvian wart. The disease is transmitted by the Phlebotomus sand fly in mountain valleys of Peru, Ecuador, and Colombia.
Lesions are small patches which give rise to bright red papules and nodules up to several centimeters in size. Hemorrhage, ulceration, and secondary infection are often associated with these lesions. If they do not become secondarily infected, the lesions will heal without scaring.
Lesions are small patches which give rise to bright red papules and nodules up to several centimeters in size. Hemorrhage, ulceration, and secondary infection are often associated with these lesions. If they do not become secondarily infected, the lesions will heal without scaring.
Cat-Scratch Disease
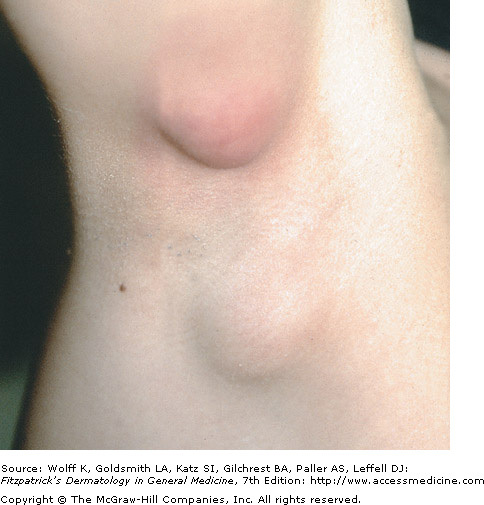
Lymphadenopathy of the Axilla - Fitzpatrick's
Cat-scratch disease is caused by an infection of Bartonella henselae. Tender regional lymphadenitis lasting many weeks to months is typical in most patients. The vast majority of patients report recent contact with cats. Go figure. Patients present with tender, visible lymph nodes measuring 1-10 cm in diameter. Usually, it is a single mobile lymph node with swelling and erythema of the overlying skin. In two-thirds of patients, a primary lesion is recognized. This could be a scratch, scar, or crusted pustule. Immunocompromised patients, such as those with HIV infection, can develop severe infections with cat-scratch disease. In patients with a normal immune system, the disease is usually self limiting.
Rocky Mountain Spotted Fever
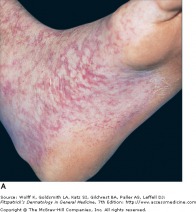
Early Macular Lesions of RMSF - Fitzpatrick's
Rocky Mountain spotted fever is caused by the organism Rickettsia rickettsi. It begins with fever, chills, headache, myalgia, malaisa, and GI symptoms 6-8 days after a tick bite. Cutaneous eruptions then occur 2-4 days after the onset of fever. The first lesions are erythematous macules localized around the wrists and ankles. This then becomes maculopapular with central petechiae. The spread is in a centripetal pattern and involves the trunk, extremities, palms, soles, and spares the face. In 10 percent of patients, the cutaneous eruption does not occur at all so treatment should be started regardless if tick exposure is suspect.
Severe cases of RMSF are characterized by multi-organ symptoms, including seizures, ataxia, neuropathy, meningitis, and cranial nerve palsies. Cough, dyspnea, and pleural effusion are common respiratory symptoms, and other organs such as the heart and liver may be involved. The mortality rate, if untreated, is 20-25 percent. Long term neurologic sequelae are also known to be associated with RMSF, so appropriate treatment is critical.
Severe cases of RMSF are characterized by multi-organ symptoms, including seizures, ataxia, neuropathy, meningitis, and cranial nerve palsies. Cough, dyspnea, and pleural effusion are common respiratory symptoms, and other organs such as the heart and liver may be involved. The mortality rate, if untreated, is 20-25 percent. Long term neurologic sequelae are also known to be associated with RMSF, so appropriate treatment is critical.
