Learning Dermatology is Learning a New Language
If you follow a dermatologist during clinic, you will probably hear a cacophony of adjectives and descriptors being exchanged among attendings, residents, and nurses. The world of dermatology can be intimidating at first, but with a basic background, you will be able to describe most skin lesions. The goal of this page is to familiarize you with the basic terminology used in dermatology, so that you may better document skin findings in the medical record, communicate with colleagues, and effectively consult with a dermatologist.
According to a study by Fleischer et al, 7% of all adult outpatient visits are for a skin complaint, while 60% of these cases are made to non-dermatologists. Being able to effectively describe and document skin lesions will be essential. Take a look at the learning module below to learn about some common lesions and their distributions, and be sure to visit the links at the bottom of the page for more information.
According to a study by Fleischer et al, 7% of all adult outpatient visits are for a skin complaint, while 60% of these cases are made to non-dermatologists. Being able to effectively describe and document skin lesions will be essential. Take a look at the learning module below to learn about some common lesions and their distributions, and be sure to visit the links at the bottom of the page for more information.
Raised Lesions
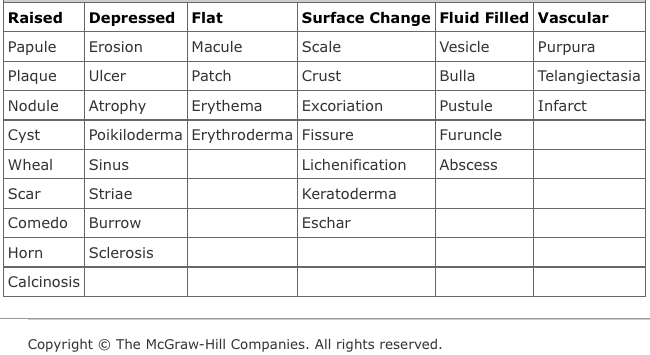
Papule
Lichen Planus - Fitzpatrick's Dermatology
A solid, elevated lesion less than 0.5 cm in size. A large proportion of a papule projects above the plane of the surrounding skin. Papules come in many shapes, some of the most common being flat-topped, domed, pedunculated, rough, smooth, filiform, acuminate(sharp-pointed), and umbilicated. To the left, you can see examples of flat-topped papules of lichen planus.
Plaque

Psoriasis Vulgaris - Fitzpatrick's Dermatology
A solid elevation over a large surface area that resembles a plateau in shape. The diameter is larger than 0.5 cm, and the elevation does not need to be a significant height. You can describe a plaque in more detail by its size, shape, color, and surface change. A common example of a plaque in dermatology is psoriasis.
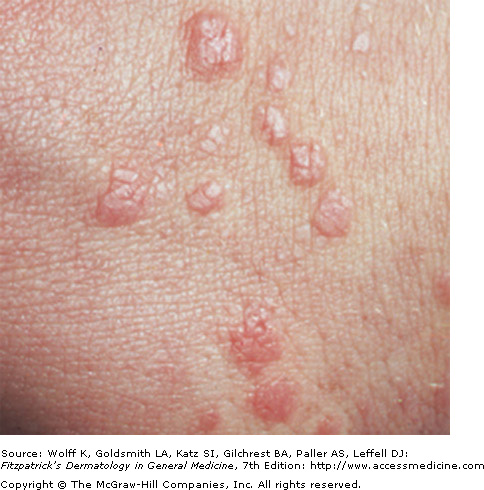
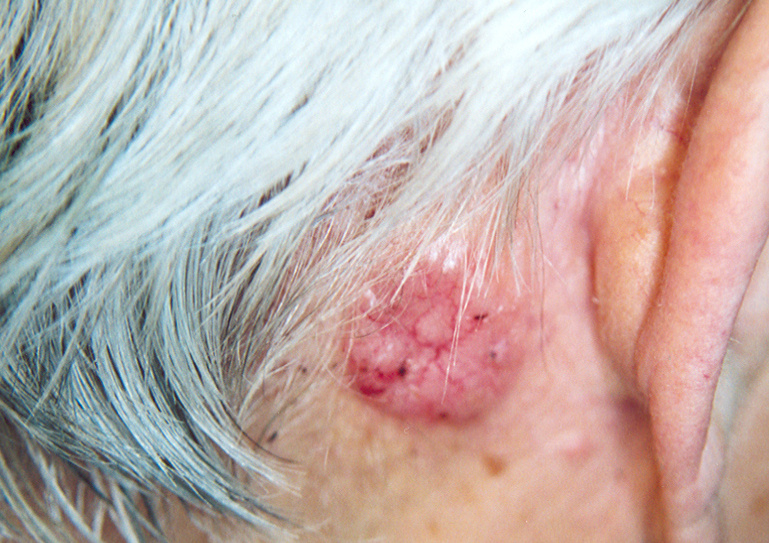
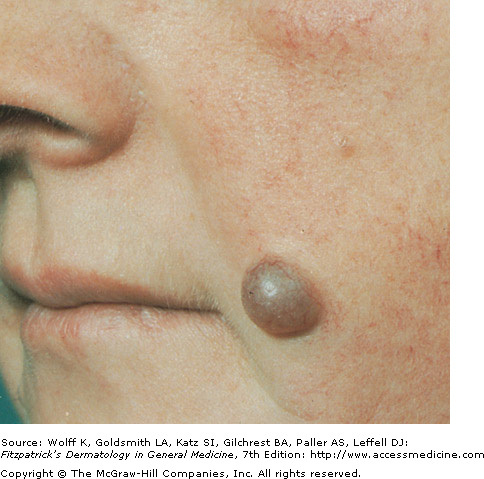
Nodule
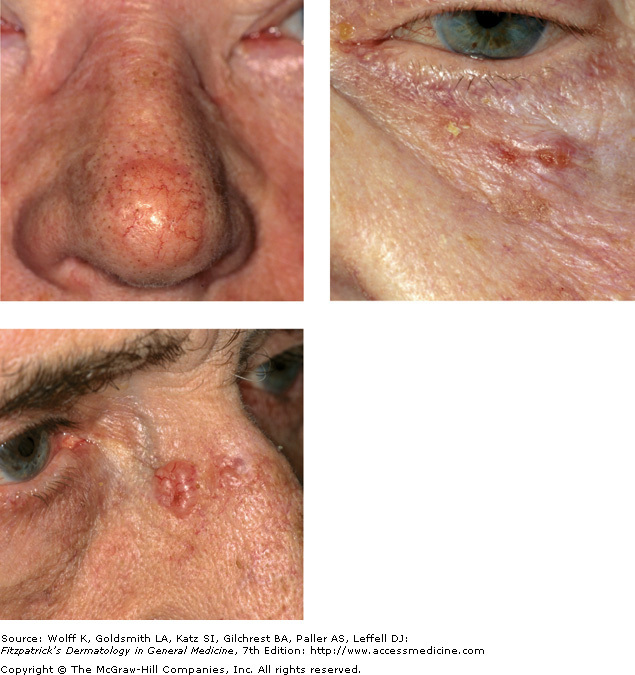
Nodular Basal Cell Carcinoma - Fitzpatrick's Dermatology
A nodule is a solid, palpable lesion larger than 0.5 cm that is round or oval shaped. Nodules are different from papules or plaques in that they have a greater depth of involvement in the skin, either as epidermal, epidermal-dermal, dermal, dermal-subdermal, or subcutaneous. They can be further described to aid in diagnosis. Examples includes nodules that are smooth, ulcerated, or fungating. Clinically, nodules can be seen in nodular basal cell carcinoma. The nodules of juvenile xanthogranuloma limited to the skin are often self-limiting and benign. Involvement of the eye has blindness as a potential complication.
 Xanthogranuloma Nodules - DermAtlas |
 Nodular Basal Cell Carcinoma - DermAtlas |
Cyst
Cystic Hidradenoma - Fitzpatrick's Dermatology
An encapsulated cavity or sac, lined with epithelium, containing fluid or a semisolid material. Due to the contents applying equal pressure over the epidermis, cysts have spherical or oval shapes. A nodule or papule may be cystic if it is resilient upon palpation. Their palpation consistency is sometimes described as feeling similar to the eyeball, however they may be hard, fluctuant, or doughy.
Wheal

Urticaria - Fitzpatrick's Dermatology
A wheal is indicative of hives or utricaria. These lesions are caused by edema in the dermis, as plasma escapes through blood vessel walls. They vary in size, ranging from tiny papules to giant plaques greater the 10 cm. The borders are sharp, however they move to different areas in the course of just hours. If fixed, vasculitis must be considered. Red or pink in color, a ring of pink erythema is often seen if superficial vessels are dilated.
Scar

Hypertrophic Scar - Fitzpatrick's Dermatology
Scars are formed when fibrous tissue replaces normal skin that was damaged by a wound or ulcer compromising the dermis. Initially, they are pink or red in color, and later may become hypo- or hyperpigmented. The epidermis is thin, and has a wrinkly appearance on the surface. Note that there is no normal hair on a scar, as these structures in the dermis have been destroyed.
Comedo (Comedones)

Open and Closed Comedo in Comedonal Acne - Fitzpatrick's Dermatology
A comedone is a dilated hair follicle that has been plugged with keratin and lipids. Open comedones (blackheads) occur when the pilosebaceous unit is open to the surface of the skin with a keratinaceous plug. Closed comedones (whiteheads) are characterized by a closed infundibulum where you cannot see the follicular opening, and contain whitish keratin. Comedones are common on the face, trunk, back, and shoulders.
Horn
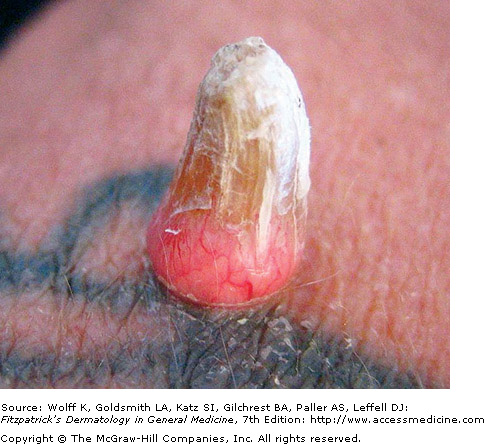
Verruca Vulgaris - Fitzpatrick's Dermatology
A horn is a conical mass of cells over an abnormally differentiating epidermis. Horns form due to an underlying pathology at the base, such as HPV infection in keratinocytes (warts), growth of mutated keratinocytes in squamous cell carcinoma, actinic keratoses, or seborrheic keratoses.
Depressed Lesions
Erosion
Toxic Epidermal Necrolysis - Fitzpatrick's Dermatology
An erosion is a circumscribed, depressed lesion resulting from the loss of a portion or all of the epidermal or mucosal epithelium. Pinpoint bleeding may occur if the lesion reaches the upper-most portion of the dermis.
Atrophy
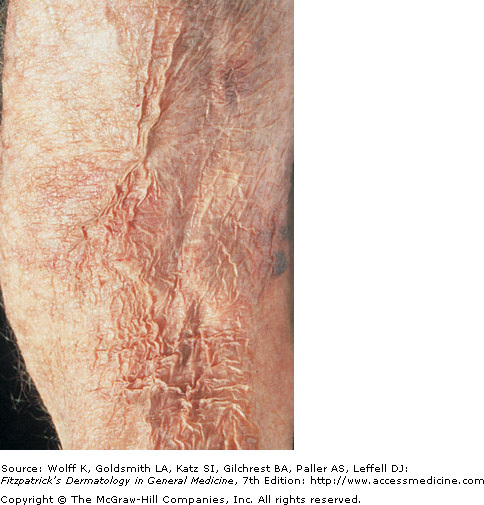
Atrophy - Fitzpatrick's Dermatology
Epidermal atrophy occurs as the number of epidermal cells decreases and results in a thinning of the epidermal layer. Its appearance is that of glossy, wrinkled paper. Normal texture of the skin is typically lost, and can be caused by chronological aging and sun damage.
Ulcer
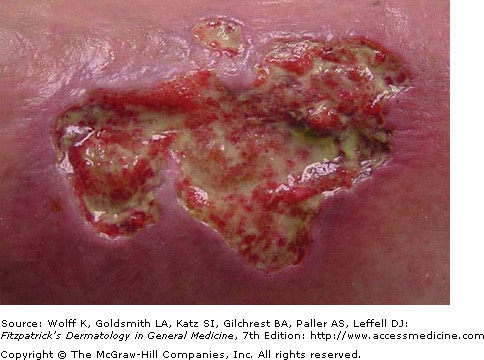
Pyoderma Gangrenosum - Fitzpatrick's Dermatology
An ulcer is a lesion in which the epidermis and parts of the dermis have been removed. Since the dermis is breached, ulcers heal with scarring. Borders may be rolled, undermined, punched out, or jagged. The base of the ulcer can range from clean to necrotic, with possible purulent discharge.
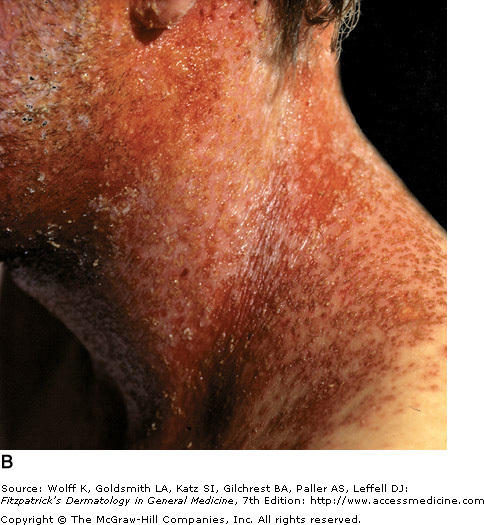
Poikiloderma

Chronic Radiodermatitis - Fitzpatrick's Dermatology
Poikiloderma is a combination of findings, including atrophy, telangiectasia, and pigmentary changes (hyper- and hypopigmentation). The appearance is dappled due to the many variations in color (think dapple gray horses).
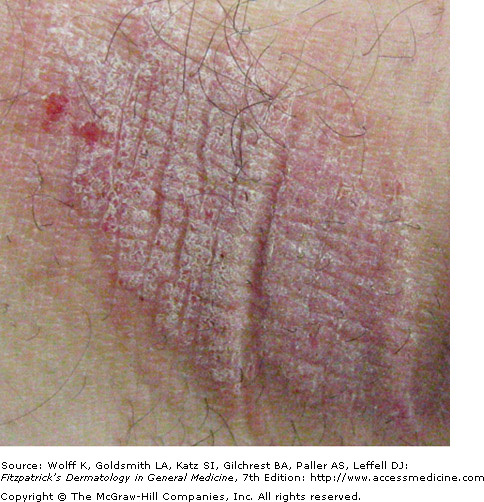
Striae

Linear Striae - Fitzpatrick's Dermatology
Striae are linear depressions of the skin several centimeters long. Also known as stretch marks, striae result from changes in reticular collagen as a result of rapid stretching of the skin. The surface can be thin and wrinkled, with a pink/red color, and will eventually become pale and flattened.
Sclerosis

Morphea - Fitzpatrick's Dermatology
Sclerosis is a circumscribed or diffuse hardening of the skin resulting from dermal fibrosis. On palpation, the skin will feel immobile and board-like. Hyper- or hypopigmentation may be present, and the epidermis over the sclerotic dermis may be atrophic. Sclerosis can reach to the deep fascia, muscle, and bone, leading to deformities and loss of function.
Flat Lesions
Macule
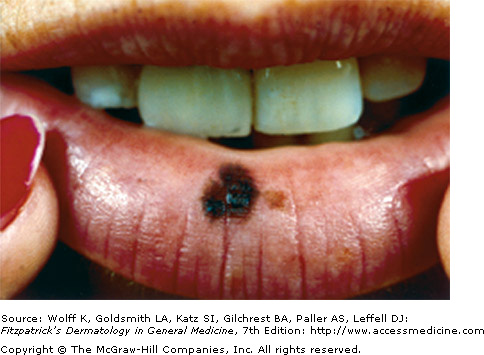
Lentigo - Fitzpatrick's Dermatology
A macule is a flat, non-palpable lesion with a color change different than the surrounding skin. Macules are less than 0.5 cm, and have varying shapes and colors, indicating different pathologies. They may be hyperpigmented, hypopigmented, or depigmented.
Patch
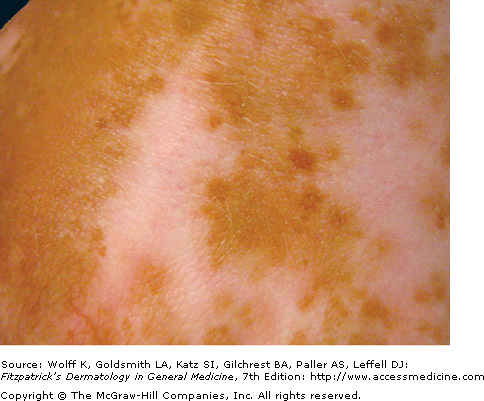
Depigmented Patch in Vitiligo - Fitzpatrick's Dermatology
A patch is similar to a macule, however it is larger than 0.5 cm. Groups of patches can cover large areas of the body, and like macules, come in a variety of shapes and colors.
Erythema
Dusky Red Erythema due to Drug Eruption - Fitzpatrick's Dermatology
Erythema ias a color change in the skin due to the dilation of blood vessels in the dermis. Unlike purpura, erythema is blanchable upon diascopy examination. When describing erythema, be sure to also describe the color it most closely resembles, as pink to violaceous, as these descriptors can lead to different differential diagnoses.
Surface Changes
Scale, Desquamation

Brittle Silvery Scales on Psoriasis - Fitzpatrick's Dermatology
Scale represents a flat plate or flaking from the outer stratum corneum. Accumulation of the stratum corneum can manifest as fine-particles or as large sheets. A clinical example of scaling occurs on plaques of psoriasis.
Crusts

Impetigo - Fitzpatrick's Dermatology
Crusts are hardened deposits from dried serum, blood, or purulent exudate on the skin. Serous secretions form a yellow-brown crust, while blood forms a reddish-black crust. Honey-colored crusts are a sign of impetigo. An erosion or ulcer may underly the crusts.
Lichenification
Lichen Simplex Chronicus - Fitzpatrick's Dermatology
Lichenification is a reactive thickening of the epidermis, resulting in changes of the collagen in the dermis. This may be caused by excessive rubbing of the skin, giving a "tree bark" appearance.
Eschar

Eschar of Deep Fungal Infection - DermAtlas
Escahrs imply tissue necrosis and are present in serious skin conditions such as gangrene and deep burns. They are circumscribed, hard, black crusts on the surface of the skin. An eschar is protein rich and is not vascular. The growth of microbes is facilitated in this environment.
Fluid-Filled Lesions
Vesicle
Impetigo from Toxin-Producing Staphylococcus - Fitzpatrick's Dermatology
Vesicles are fluid-filled cavities or elevations smaller than 0.5 cm, and bullae are larger than 0.5 cm. The equal pressure distribution of the fluid gives vesicles and bullae their round appearance. The contents of these lesions may be clear, serous, hemorrhagic, or pus filled.
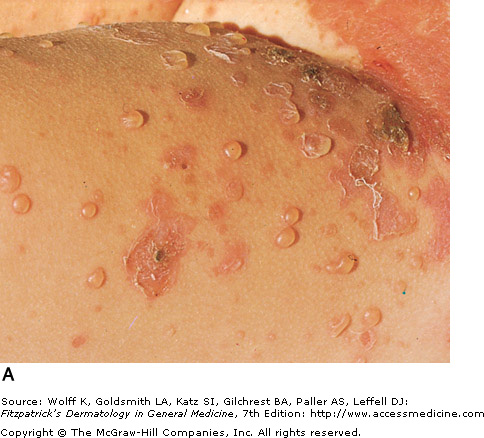
Bulla
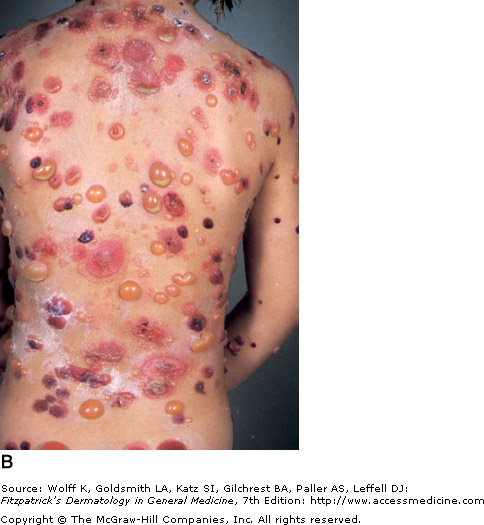
Bullous Pemphigoid - Fitzpatrick's Dermatology
A bulla is an overgrown vesicle, measuring greater than 0.5 cm.
Pustule
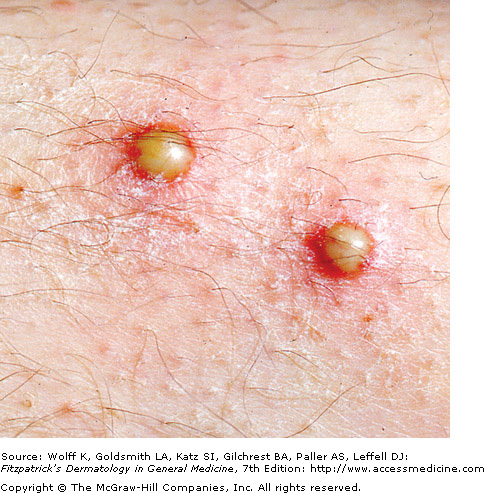
Superficial Pyoderma - Fitzpatrick's Dermatology
A pustule is a circumscribed, raised cavity in the epidermis that contains pus. The purulent exudate contains leukocytes, may or may not contain cell debris, and may contain bacteria or be sterile. There may be a red erythematous ring around the pustule, but this will not scar, as the dermis is not involved. Post-inflammatory pigmentary changes may occur.
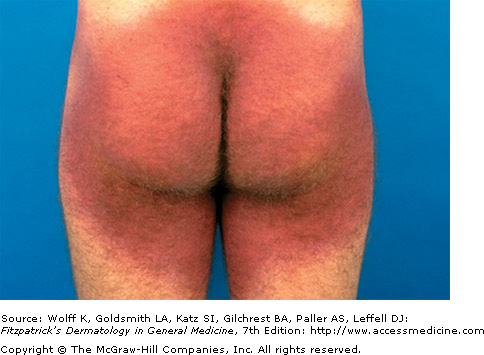
Abscess

Red Erythematous Abscess on Leg - Fitzpatrick's Dermatology
An abscess is a localized accumulation of purulent material deep in the dermis or subcutaneous tissue. Due to its depth, the pus is not typically visible on the surface until it is ready to drain. It is a nodule that is warm, tender, and fluctuant. Common causes of abscesses in the skin are due to staph infection.
Vascular Lesions
Purpura

Leukocytoclastic Vasculitis - Fitzpatrick's Dermatology
Purpura are caused by the extravasion of blood (outside the cutaneous vessels) leading to red/purple lesions. Using diascopy (blanching test with a glass slide), purpura do not blanch and maintain their color and form. Small, pinpoint purpuric macules are called petechiae. Larger purpuric lesions are called ecchymoses (bruises). The color of the lesions changes over time with the decomposition of red blood cells.
Telangiectasia

Dilated Superficial Capillaries of Telangiectasia - Fitzpatrick's Dermatology
Telangiectasia are persistent dilations of small capillaries in the superficial dermis. They can be realized as fine red lines on the skin. These lesions may or may not blanch with diascopy.
Shape and Distribution of Lesions
Identifying the type of lesion is very important, but this is only half the battle. Next, describe the shape, arrangement, and pattern of distribution of the lesions for a more complete morphology.
Shapes of Skin Lesions
Shapes of Skin Lesions
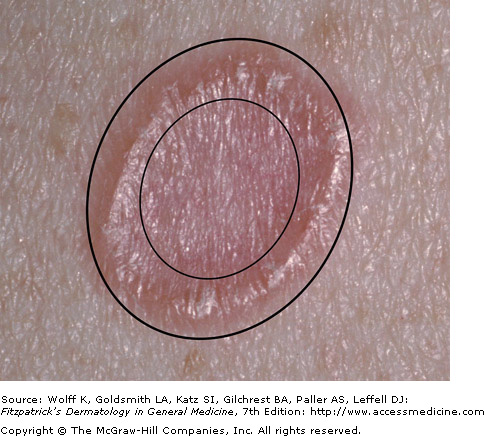
- Annular: ring shaped, edge of the lesion differs from the center
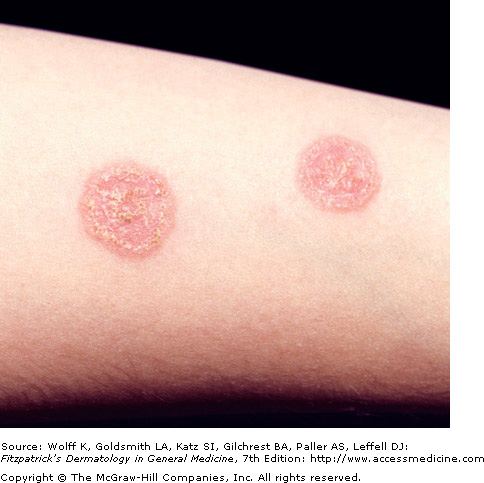
- Round/nummular/discoid: round or oval shaped, uniform from the edges to the center
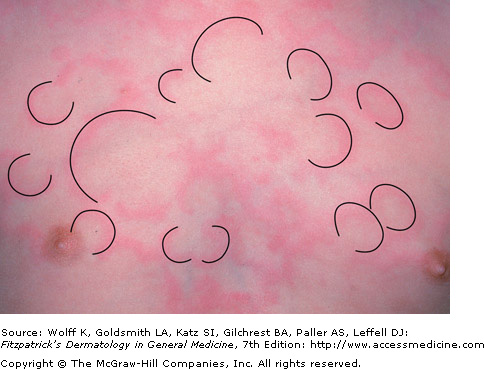
- Polycyclic: coalescing circles, rings, or incomplete rings
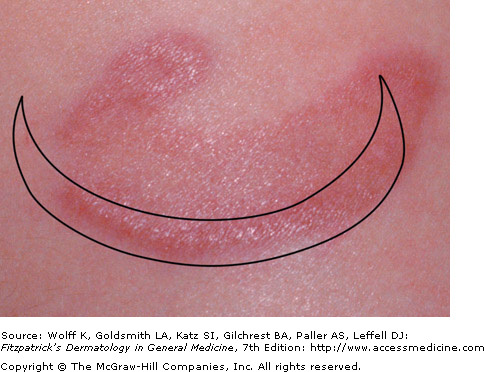
- Arcuate: arc-shaped, may be an incomplete annular lesion
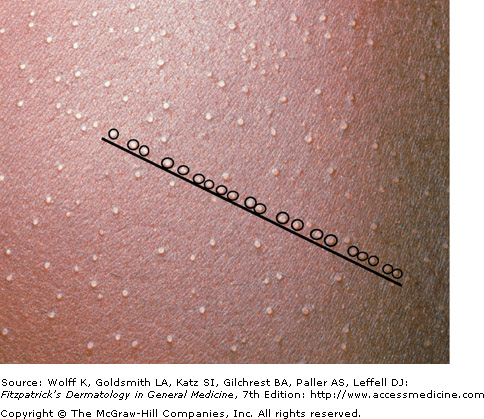
- LInear: may refer to one lesion, or multiple lesions lined up in a straight line
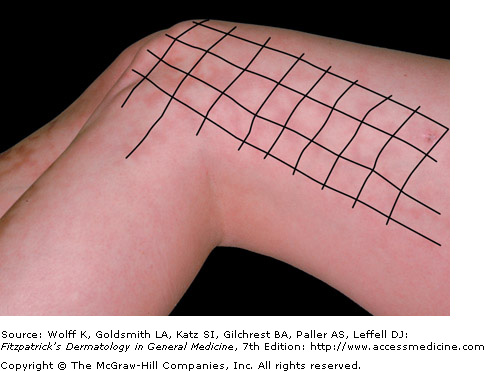
- Reticular: net-like or lacey, with regularly spaced rings/partial rings
- Serpiginous: snake-like curving lesion in a wandering pattern
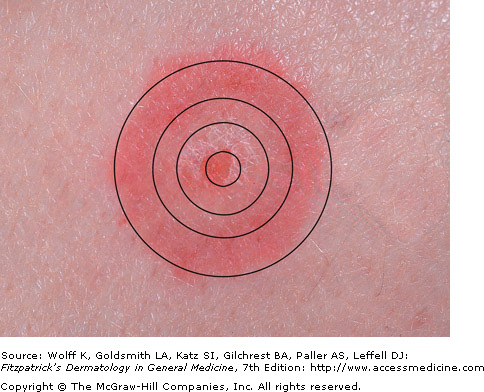
- Targetoid: in the shape of a bulls-eye target, at least three distinct zones
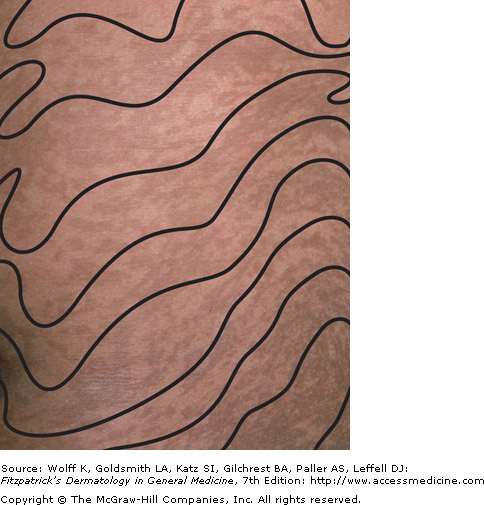
- Whorled: marble-like appearance with distinct colors in a wavy pattern
- Grouped (Herpetiform): clustered together, similar to the classic appearance of HSV 1
- Scattered: irregularly distributed lesions
- Dermatomal (Zosteriform): lying in the distribution of a signal dermatome, like the classic presentation of herpes zoster
- Lymphangitic: lying along the drainage of a lymph vessel
- Sun Exposed: in areas that are typically not covered by clothing, such as the face and hands
- Sun Protected: in areas that are covered by clothing
- Acral: occuring in distal locations (hands, feet, ankles, wrists)
- Truncal: occuring on the central body
- Extensor: occuring on dorsal extremities, overlying extensor muscles, knees, and elbows
- Flexor: overlying flexor muscles, antecubital fossae, popliteal fossae
- Intertriginous: occuring in the skin folds, areas where two skin surfaces are in contact
Shape Images - Please Click to Reveal Description:

Websites for Interactive Learning of Skin Morphology:
 Interactive Terms with Images from the Dermatology Lexicon Project |
 Interactive Activities on the Skin Exam and Describing Lesions |
References
- Fleischer AB Jr, Feldman SR, McConnell RC. The most common dermatologic problems identified by family physicians, 1990-1994. Family Medicine. 1997 Oct;29(9):648-52.
- Garg Amit, Levin Nikki A, Bernhard Jeffrey D, "Chapter 4. Structure of Skin Lesions and Fundamentals of Clinical Diagnosis" (Chapter). Wolff K, Goldsmith LA, Katz SI, Gilchrest B, Paller AS, Leffell DJ: Fitzpatrick's Dermatology in General Medicine, 7e.
- Dermatology Atlas. Bernard A. Cohen, MD, Christoph U. Lehmann, MD, DermAtlas, Johns Hopkins University; 2000-2010 . Available at: http://dermatlas.med.jhmi.edu/derm/
