Cardiac and Pulmonary Disease
Endocarditis - Bacterial and Fungal
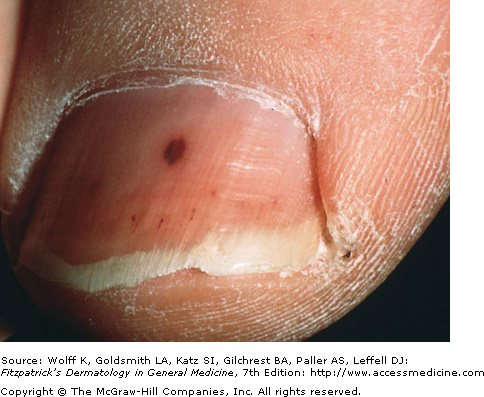
Splinter Hemorrhage
Endocarditis causes bacterial or fungal growths on or near the heart valves. There are many cutaneous signs, and in context can aid in the diagnosis of endocarditis. Infection with gram-positive bacteria may lead to sepsis, causing syndromes such as disseminated intravascular coagulation (DIC), leading to additional skin symptoms.
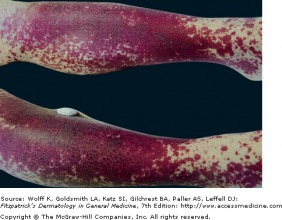
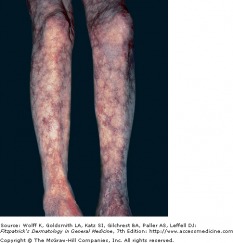
-Purpura: many petichiae are seen in the extremities and soft palate.
-Splinter hemorrhage: 1-2 mm, red-brown streaks in the nail plate due to small emboli or capillary vasculits. They are present in about 15% of endocarditis patients.
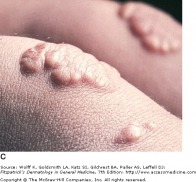
-Janeway lesions: painless, erythematous maculopapules on the palms and soles that do not blanche. They are caused by thrombi in small vessels, without vasculitis.
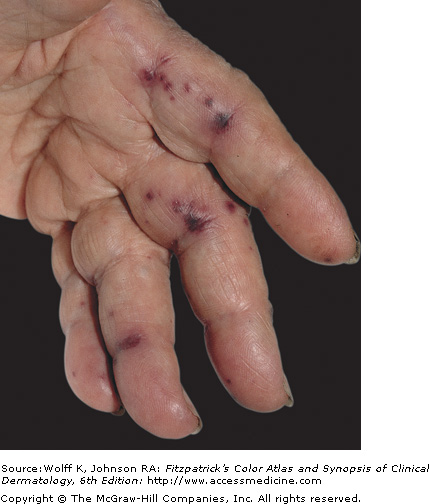
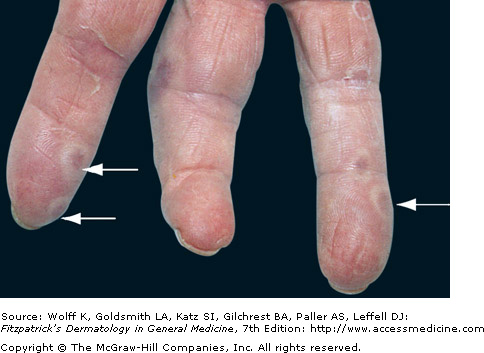
-Osler's nodules: painful, red papulo-nodules with a pale center. They are found on the fingertips, and last days to weeks. Caused by microabscesses in the dermis, they may even contain gram-positive cocci.
-Purpura: many petichiae are seen in the extremities and soft palate.
-Splinter hemorrhage: 1-2 mm, red-brown streaks in the nail plate due to small emboli or capillary vasculits. They are present in about 15% of endocarditis patients.
-Janeway lesions: painless, erythematous maculopapules on the palms and soles that do not blanche. They are caused by thrombi in small vessels, without vasculitis.
-Osler's nodules: painful, red papulo-nodules with a pale center. They are found on the fingertips, and last days to weeks. Caused by microabscesses in the dermis, they may even contain gram-positive cocci.
 Janeway Lesions - Fitzpatrick's Dermatology |
 Osler's Nodes - Fitzpatrick's Dermatology |
Hyperlipidemia
Xanthoma of Familial Hypercholesterolemia
Excessive VLDL and LDL cholesterol levels in circulation can manifest as cutaneous xanthomas of many different varieties. Xanthomas are typically plaques or nodules, and they are caused by abnormal deposits of lipid and foam cells. Hereditary conditions such as familial chylomicronemia syndrome (Frederickson Type I) and Hypercholesterolemia (Frederickson Type II) can exacerbate high lipid levels and are associated with different types of xanthomas. Depending on the underlying condition, dietary modification (good luck) and statin drugs (HMG-coenzyme A reductase inhibitors) can be effective in preventing xanthomas.
Vasculitis

Utricarial Vasculitis - Fitzpatrick's Derm
Systemic vaculitis is an inflammatory condition in which blood vessels are subjected to an inflammatory reaction. Many organs are typically involved, including the skin. Vasculitis has many cutaneous manifestations, including palpable purpura, fixed urticaria (hives), ulcers, ischemia of the fingers, and livedo reticularis (lace-like pattern of purpura on the lower extremities). Vasculitis can be secondary to conditions such as giant cell arteritis, hypercoagulability, Raynaud's, Marfan syndrome, or other processes, like atherosclerosis, that inflame vessel walls. When other causes have been excluded, vasculitis may be classified as a primary process.
 Leukocytoclastic Vasculitis |
 Livedo Reticularis - Fitzpatrick's Dermatology |
Tuberculosis
TB Verrucosa Cutis - Fitzpatrick's Dermatology
Tuberculosis is so wide-spread, it is estimated that one-third of the world's population is infected. It affects the lungs, but nearly any other organ can be affected. Cutaneous manifestations are generally rare with Mycobacterium tuberculosis infection, however there a are wide variety of findings. Other mycobacteria species produce skin lesions more often than Mycobacterium tuberculosis.
The following list shows the different skin findings associated with each respective subtype of tuberculosis:
Primary Inoculation Tuberculosis: Children are most affected in the locations of the face, hand, and lower extremities. A chancre appears 2-4 after innoculation, which then develops into a painless ulcer. Weeks later, regional lymphademopathy develops, and eventually cold abscesses may develop, perforating the skin and forming sinuses.
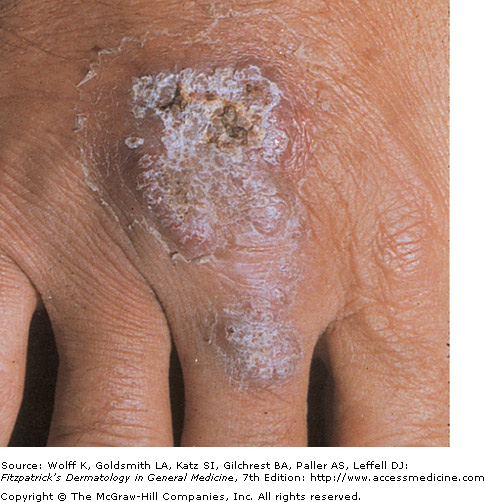
Tuberculosis Verrucosa Cutis (Warty Tuberculosis): This is caused when individuals who had a previous TB infection with high-immunity get an exogenous re-infection. Lesions become hyperkeratotic and often look like a common wart. Slow growth leads to a verrucous plaque and irregular border, with fissures discharging pus. They can persist for many years if left untreated.
Lupus Vulgaris: A chronic form of cutaneous tuberculosis, LV infections occur in patients with moderate immunity and a high tuberculin sensitivity. The lesions are usually in a single location on the head and neck, however multiple sites could be involved simultaneously. Initially the lesion presents as a brown-red soft or friable macule or papule with hyperkeratosis. It has an apple jelly color on diascopy (pressing a glass slide against the skin). Later on, the lesion is elevated, forms a plaque, and may ulcerate.
The following list shows the different skin findings associated with each respective subtype of tuberculosis:
Primary Inoculation Tuberculosis: Children are most affected in the locations of the face, hand, and lower extremities. A chancre appears 2-4 after innoculation, which then develops into a painless ulcer. Weeks later, regional lymphademopathy develops, and eventually cold abscesses may develop, perforating the skin and forming sinuses.
Tuberculosis Verrucosa Cutis (Warty Tuberculosis): This is caused when individuals who had a previous TB infection with high-immunity get an exogenous re-infection. Lesions become hyperkeratotic and often look like a common wart. Slow growth leads to a verrucous plaque and irregular border, with fissures discharging pus. They can persist for many years if left untreated.
Lupus Vulgaris: A chronic form of cutaneous tuberculosis, LV infections occur in patients with moderate immunity and a high tuberculin sensitivity. The lesions are usually in a single location on the head and neck, however multiple sites could be involved simultaneously. Initially the lesion presents as a brown-red soft or friable macule or papule with hyperkeratosis. It has an apple jelly color on diascopy (pressing a glass slide against the skin). Later on, the lesion is elevated, forms a plaque, and may ulcerate.
Sarcoidosis
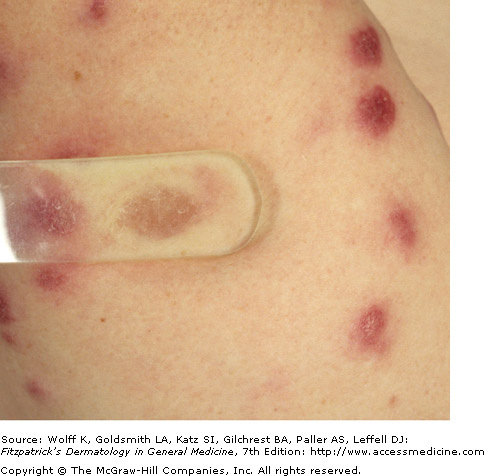
Apple Jelly Color of Sarcoidosis on Diascopy
Sarcoidosis is a systemic granulomatous disease that affects the lungs, but can also affect the skin. Worldwide it is most prevalent in Scandinavia. Acutely, it presents clinically as erythema nodosum, most commonly affecting the head and neck. In chronic cases, it takes on a papular form, characterized by translucent yellow-red papules with an apple jelly appearance on diascopy. On biopsy, noncaseating granulomas serve as further evidence in diagnosis, however they are not specific. Sarcoid has many clinical presentations and the examiner needs to be aware of its many presentations.
Blastomycosis
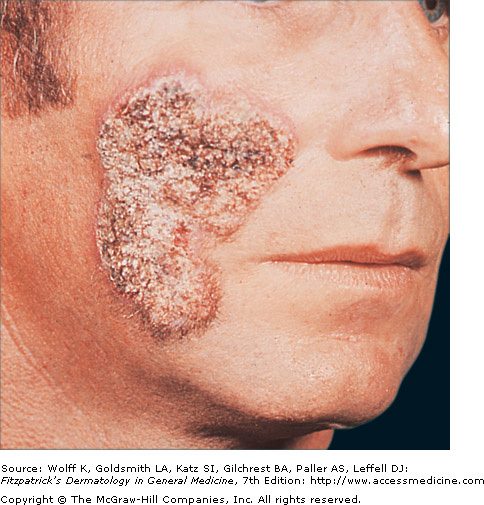
Verrucous Plaque on Cheek - Fitzpatrick's Dermatology
Blastomycosis is a chronic fungal infection primarily affecting the lungs, but also disseminating to involve the skin, bones, and CNS. It is most common in the Great Lakes regions of the U.S. and Canada, as well as in the southern states.
The lesions are characterized as verrucous, ulcerating plaques or nodules.
Lesions in some cases may be studded with pustules. The face and extremities are most affected, and distribution is often symmetric. In clinical presentation, blastomycosis has similar respiratory symptoms as pulmonary tuberculosis. Skin lesions are often used to aid in the diagnosis of disseminated disease.
The lesions are characterized as verrucous, ulcerating plaques or nodules.
Lesions in some cases may be studded with pustules. The face and extremities are most affected, and distribution is often symmetric. In clinical presentation, blastomycosis has similar respiratory symptoms as pulmonary tuberculosis. Skin lesions are often used to aid in the diagnosis of disseminated disease.
 Chromoblastomycosis - patient was on long-term steroids |
 Ulcerating Chromoblastomycosis |
