History

While dermatology is a very visual discipline, a good history is often beneficial. In practice, clinicians often perform a brief visual exam of the patient's chief complaint, followed by a focused history, and then a more extensive examination. The patient's history should include a complete characterization of the lesion or condition in question. This description should include symptoms (including itching, pain, burning), intensity, duration, alleviating factors, aggravating factors, and the initial site of the lesion. The natural history of the condition should also be established through a chronology of any changes. Furthermore, it is important to inquire about any exposures, systemic diseases, injuries, and current medications. A family history of important conditions, such as skin cancers, and a social history should be included. During the physical exam, you can clarify responses and ask additional history. Finally, the patient's health literacy and expectations regarding treatment outcomes should be assessed and considered when developing the treatment plan.
Physical Exam - General Considerations
The chief element in the examination of the skin is inspection. Visual inspection can be supplemented by various magnification and illumination tools. Palpation is used to appreciate many characteristics, including nodularity, induration, heat, and texture. When visualization and touch are combined, it becomes a powerful diagnostic tool.
The complete skin exam should be performed systematically, so as not to overlook any areas. Ideally, the patient should be fitted in a gown prior to beginning the exam. Patient modesty should be preserved throughout the visit. Clinicians vary in their styles of approach to the systematic skin exam. Two popular methods are moving from the head all the way down to the feet, or beginning at the extremities of the hands and arms and moving inwards towards the trunk. Regardless of the starting point, consistency is key.
An appreciation for what is normal is necessary when looking for abnormalities of the skin. Individuals can have considerable normal variation. Pathologic conditions often change over time, and examination may be complicated by normal signs of aging. Chronic disease may have cutaneous manifestations, and light-skinned individuals may show certain lesions differently than dark-skinned patients. Overall, it is the patient, not just the skin, that needs to be examined the context of the history and presentation.
The complete skin exam should be performed systematically, so as not to overlook any areas. Ideally, the patient should be fitted in a gown prior to beginning the exam. Patient modesty should be preserved throughout the visit. Clinicians vary in their styles of approach to the systematic skin exam. Two popular methods are moving from the head all the way down to the feet, or beginning at the extremities of the hands and arms and moving inwards towards the trunk. Regardless of the starting point, consistency is key.
An appreciation for what is normal is necessary when looking for abnormalities of the skin. Individuals can have considerable normal variation. Pathologic conditions often change over time, and examination may be complicated by normal signs of aging. Chronic disease may have cutaneous manifestations, and light-skinned individuals may show certain lesions differently than dark-skinned patients. Overall, it is the patient, not just the skin, that needs to be examined the context of the history and presentation.
Performing and Documenting the Skin Exam
The complete skin exam is needed to establish a baseline at the beginning of care. While often not necessary for every presenting concern, it should be used in screening for important conditions such as melanoma and other skin cancers. A systematic method is used to ensure that no parts of the skin are overlooked. Components of the complete exam include the entire skin surface (including the scalp, eyelids, ears, genitals, buttocks, perineal area, and interdigital spaces), the hair, the nails, and the mucus membranes.
Upon finding an abnormality, the clinician must now be able to describe what they see. For this purpose, dermatologists use a seemingly foreign language of terms and descriptions. Knowing the basics of describing your observations is key when consulting with dermatologists and other physicians. If you can describe a condition over the phone to a dermatologist colleague, they may be able to determine that a consultation
is not necessary, and the condition can be managed in the primary care clinic. This saves the patient time and money, and allows for better allocation of health care resources.
Documenting abnormalities should be done using the following sequence of observations:
Photographs are also very useful in documenting skin conditions. As lesions often change over time, photos can be a useful tool to track the disease progression and response to therapy.
Mucous Membranes
Mucous membranes can offer clues to the patient's general health. For example, abnormalities may be found in pigmentation, color, texture, lesions, and hydration in the mouth. A dry mouth can indicate dehydration, a drug side-effect, or a sign of Sjogren's syndrome. Many skin diseases affect the oral and genital mucous membranes, and some such as condyloma and candidiasis may involve only the mucosa and may be missed on improper examination.
Hair
We are know that hair has considerable variation in its color, texture, and distribution. Hair can also provide clues to both systemic and local diseases upon examination, and should not be overlooked. There are two primary types of hairs: vellus and terminal. Vellus hairs are found all over the body and are small (not longer than 1-2 cm), soft, and lightly colored. Terminal hairs are found on the scalp, beard, and other locations where hair is darker pigmented, coarse, and long. The growth of terminal hair is hormonally regulated, with androgens responsible for the conversion of some vellus hairs on the face, axilla, and groin into terminal hairs. Examination includes noting the quality, presence, and distribution of the hair in the context of the individual. Patients with abnormally higher than expected distributions of hair are said to have hypertrichosis, while hirsutism described a growth and distribution of terminal hairs in a male-like pattern on a female patient. Concern for hair loss or other changes in hair require an evaluation including a detailed history and often laboratory assessment needed for proper diagnosis.
Nails
The entire nail unit should be examined for appearance, ridges, cracks, whitening, pigment and color changes, and texture. Thickness should also be noted, and the angle at which the nail plate enters the proximal nail fold (Lovibond's angle) should be less than 180 degrees (a larger angle may indicate clubbing). Please see the diagram below for nail abnormalities.
Upon finding an abnormality, the clinician must now be able to describe what they see. For this purpose, dermatologists use a seemingly foreign language of terms and descriptions. Knowing the basics of describing your observations is key when consulting with dermatologists and other physicians. If you can describe a condition over the phone to a dermatologist colleague, they may be able to determine that a consultation
is not necessary, and the condition can be managed in the primary care clinic. This saves the patient time and money, and allows for better allocation of health care resources.
Documenting abnormalities should be done using the following sequence of observations:
- The anatomic distribution of the lesions.
- The configuration of the groups of lesions, if applicable.
- The morphology of the individual lesions.
Photographs are also very useful in documenting skin conditions. As lesions often change over time, photos can be a useful tool to track the disease progression and response to therapy.
Mucous Membranes
Mucous membranes can offer clues to the patient's general health. For example, abnormalities may be found in pigmentation, color, texture, lesions, and hydration in the mouth. A dry mouth can indicate dehydration, a drug side-effect, or a sign of Sjogren's syndrome. Many skin diseases affect the oral and genital mucous membranes, and some such as condyloma and candidiasis may involve only the mucosa and may be missed on improper examination.
Hair
We are know that hair has considerable variation in its color, texture, and distribution. Hair can also provide clues to both systemic and local diseases upon examination, and should not be overlooked. There are two primary types of hairs: vellus and terminal. Vellus hairs are found all over the body and are small (not longer than 1-2 cm), soft, and lightly colored. Terminal hairs are found on the scalp, beard, and other locations where hair is darker pigmented, coarse, and long. The growth of terminal hair is hormonally regulated, with androgens responsible for the conversion of some vellus hairs on the face, axilla, and groin into terminal hairs. Examination includes noting the quality, presence, and distribution of the hair in the context of the individual. Patients with abnormally higher than expected distributions of hair are said to have hypertrichosis, while hirsutism described a growth and distribution of terminal hairs in a male-like pattern on a female patient. Concern for hair loss or other changes in hair require an evaluation including a detailed history and often laboratory assessment needed for proper diagnosis.
Nails
The entire nail unit should be examined for appearance, ridges, cracks, whitening, pigment and color changes, and texture. Thickness should also be noted, and the angle at which the nail plate enters the proximal nail fold (Lovibond's angle) should be less than 180 degrees (a larger angle may indicate clubbing). Please see the diagram below for nail abnormalities.
Supplemental Tools in Diagnosis
There are many tools of the trade in dermatology that help the physician gain more insight when performing the physical exam. Although not an exhaustive list, below you will find some of the techniques used to establish a diagnosis.
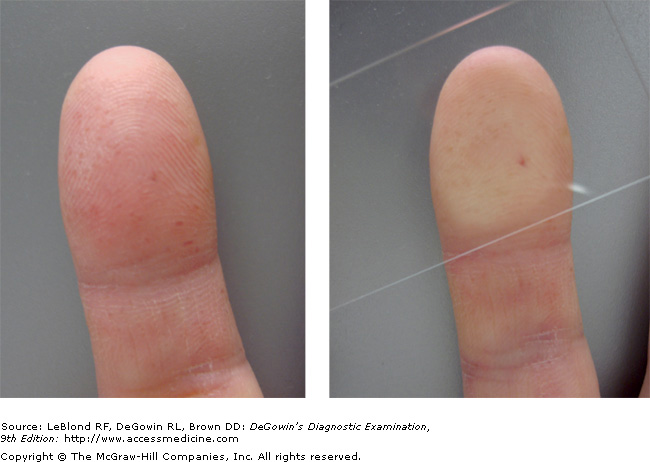
Diascopy. This is performed using a glass slide pressed against the skin to test for blanching. Blanching indicates dilated blood vessels, while extravasated blood will not blanch. In this image, petechiae are confirmed, as the blood is outside of the vessel, causing a non-blanching lesion. This means that upon pressure form the glass slide, the redness does not temporarily disappear.

Magnification. A simple magnifying glass, or moreso a lighted dermatoscope can be helpful in determining lesion morphology and features.

Woods Light. Ultraviolet light at 360 nm causes characteristic color fluorescence in some skin infections. Yellow fluorescence is often caused by fungal dermatophytes, while Pseudomonas species show a pale blue color. Corynebacterium minutissimum infections can show coral red. False negatives upon Woods Light exam are more common after a patient has bathed, as there is less fluorescent substance present on the skin.
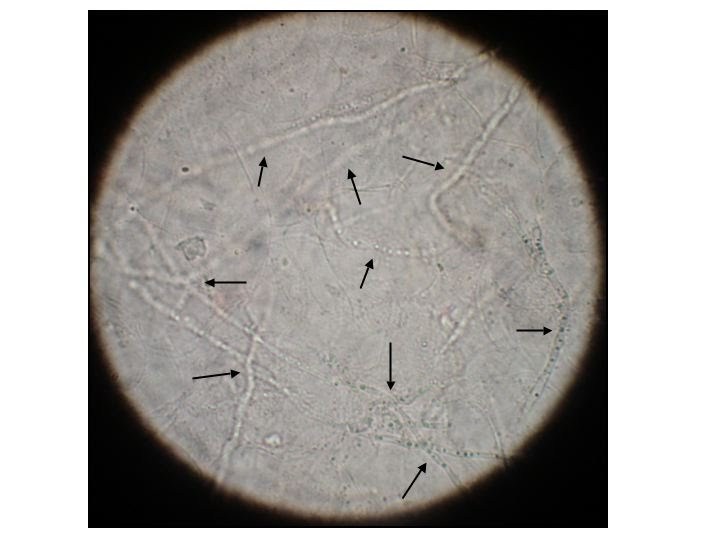
KOH Preparation. A KOH prep allows for the microscopic visualization of hyphae from dermatophyte infection. Some common specimens include candida and tinea versicolor. A sample is scraped from the lesion, and prepared on a microscope slide with KOH or chlorazole blue to dissolve keratin, allowing fungal elements to be more easily seen. Hyphae appear as thin, elongated filaments, an example of which can be seen in this image.
References:
- Schwarzenberger, K. The Essential of the Complete Skin Examination. Medical Clinics of North America. 82:5 September 1998.
- Garg Amit, Levin Nikki A, Bernhard Jeffrey D, "Chapter 4. Structure of Skin Lesions and Fundamentals of Clinical Diagnosis" (Chapter). Wolff K, Goldsmith LA, Katz SI, Gilchrest B, Paller AS, Leffell DJ: Fitzpatrick's Dermatology in General Medicine, 7e.
- LeBlond RF, Brown DD, DeGowin RL, "Chapter 6. The Skin and Nails" (Chapter). LeBlond RF, Brown DD, DeGowin RL: DeGowin's Diagnostic Examination, 9e.
