Human Papillomavirus

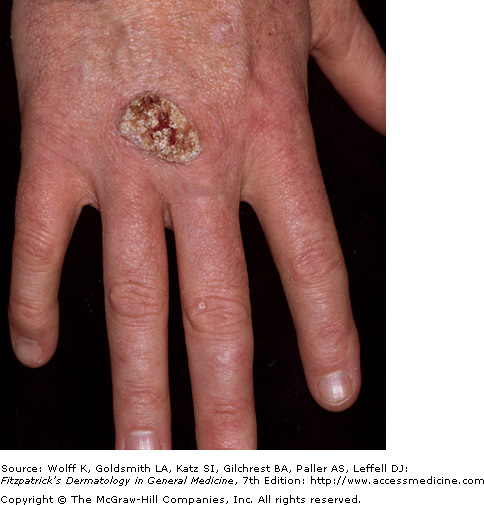
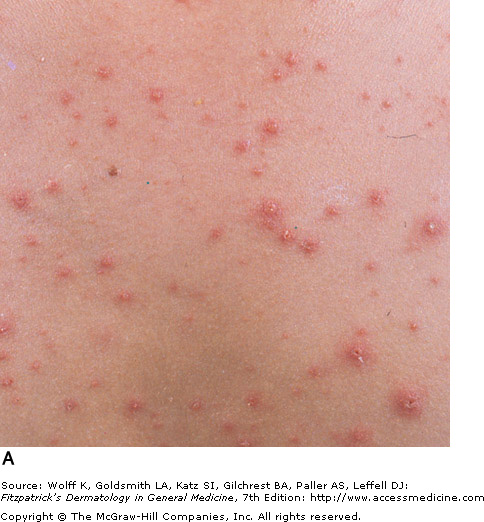
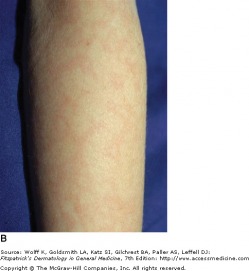
Common flat-topped warts
Human papillomaviruses are DNA tumor viruses infecting the epithelia of skin or mucosa, commonly causing warts or benign papillomas. Verrucae, commonly known as warts, are benign proliferations of skin caused by papillomavirus infection. Rather than acute signs of infection, the viruses produce a slow, focal expansion of epithelial cells with surface hyperkeratosis. Subsets of HPV infection are associated with cerival, penile, anal, and epithelial malignancies.
Verruca patients typically present with a history of a slowly expanding, scaly lesion. Over the course of several weeks to months, new lesions in the same location is suggestive of local spread of HPV infection. Common warts (verruca vulgaris) are scaly, rough, shiny papules that may erupt on any cutaneous surface. Under magnification, some warts show brown or red spots indicating thrombosed capillaries. Flat warts are elevated, flat topped papules measuring 1-4 mm in diameter, and occur most frequently on the face, hands, and lower legs. Plantar and palmar warts may be painful with pressure. They are thick, endophytic papules, and may coalesce into mosaic warts, forming large plaques.
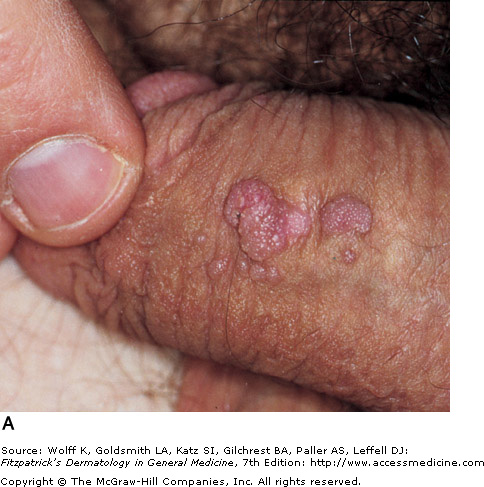
Anogenital warts are epidermal and dermal papules or nodules on the genitalia, perineum, or crural folds. They are most commonly caused by HPV-6 and HPV-11, which are considered "low risk" types with regards to invasive cancer. In the moist environment, they may form large, cauliflower-like masses. Warts may even extend inward into the vaginal canal, urethra, and rectum.
High risk HPV subtypes, such as HPV-16, HPV-18, and HPV-31are the major cause of cervical cancers. The human papillomavirus quadrivalent vaccine Gardasil offers an immunization against HPV types 6, 11, 16, and 18.
The treatment of warts depends on the patient's level of discomfort (either physical or cosmetic) and their desire for treatment. Most treatments focus on destroying the infected cells, and recurrences may occur. Cryotherapy is a common and effective treatment for most warts, in which liquid nitrogen is applied to the skin for two freeze-thaw cycles. The duration of freeze varies with location, thickness of lesion, and skin type of the patient. Potential scarring, hypopigmentation, hyperpigmentation, pain, and blistering should be discussed prior to treatment. Warts may also be debulked through surgical methods and paring. Topical therapies as cantharidin may be applied in the offce. Topicals as salycylic acid and duct tape should be utilized in between more aggressive treatments.
Verruca patients typically present with a history of a slowly expanding, scaly lesion. Over the course of several weeks to months, new lesions in the same location is suggestive of local spread of HPV infection. Common warts (verruca vulgaris) are scaly, rough, shiny papules that may erupt on any cutaneous surface. Under magnification, some warts show brown or red spots indicating thrombosed capillaries. Flat warts are elevated, flat topped papules measuring 1-4 mm in diameter, and occur most frequently on the face, hands, and lower legs. Plantar and palmar warts may be painful with pressure. They are thick, endophytic papules, and may coalesce into mosaic warts, forming large plaques.
Anogenital warts are epidermal and dermal papules or nodules on the genitalia, perineum, or crural folds. They are most commonly caused by HPV-6 and HPV-11, which are considered "low risk" types with regards to invasive cancer. In the moist environment, they may form large, cauliflower-like masses. Warts may even extend inward into the vaginal canal, urethra, and rectum.
High risk HPV subtypes, such as HPV-16, HPV-18, and HPV-31are the major cause of cervical cancers. The human papillomavirus quadrivalent vaccine Gardasil offers an immunization against HPV types 6, 11, 16, and 18.
The treatment of warts depends on the patient's level of discomfort (either physical or cosmetic) and their desire for treatment. Most treatments focus on destroying the infected cells, and recurrences may occur. Cryotherapy is a common and effective treatment for most warts, in which liquid nitrogen is applied to the skin for two freeze-thaw cycles. The duration of freeze varies with location, thickness of lesion, and skin type of the patient. Potential scarring, hypopigmentation, hyperpigmentation, pain, and blistering should be discussed prior to treatment. Warts may also be debulked through surgical methods and paring. Topical therapies as cantharidin may be applied in the offce. Topicals as salycylic acid and duct tape should be utilized in between more aggressive treatments.
|
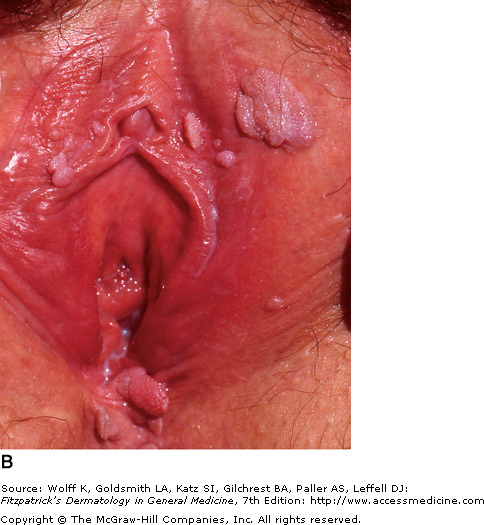 Multiple confluent condyloma on the labia minora, majora, and fourchette |
Herpes Simplex Viruses

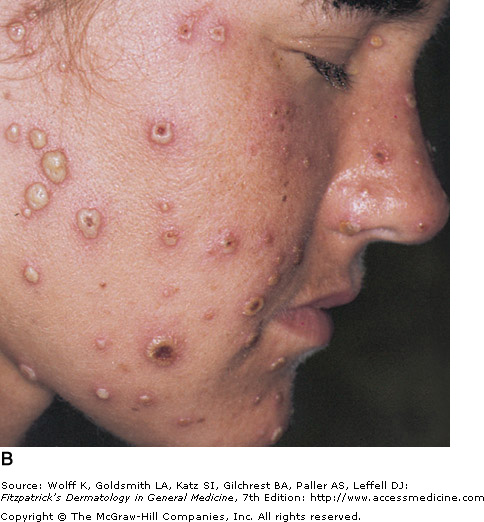
Recurrent HSV-1
Herpes simplex viruses are extremely common DNA viruses. HSV-1 is spread primarily through direct contact with contaminated saliva or secretions, while HSV-2 is spread primarily by sexual contact. Either virus however may be causal in both areas. The virus replicates at the site of infection, then travels to the dorsal root ganglia, and become latent. The virus may reactivate spontaneously, or in response to a trigger, such as UV light or immunosuppression.
Patients with HSV infection present with a highly variable clinical findings. Lesions in primary infections are initially painful vesicles on an erythematous base. They then progress to pustules and/or ulcerations. It is common to see multiple scattered vesicles, most commonly around the mouth and lips in HSV-1. Lesions will typically crust over and resolve within 2-6 weeks. Lesions occurring after the initial infection are typically less severe and fewer in number. It is not necessary for a person to have a known primary outbreak in order for them to have a latent HSV infection, as asymptomatic infection is common.
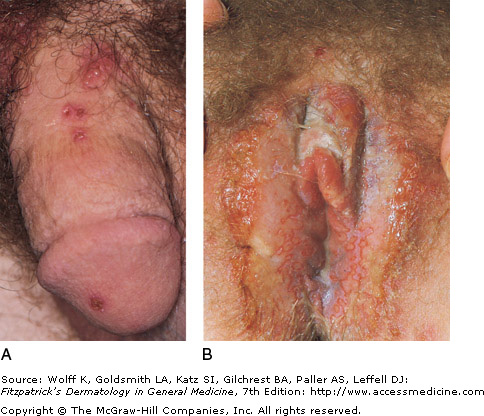
Genital herpes (HSV-2) usually produces very painful inflammation of the genitalia but may be more pruritic, especially in milder recurrent infections in males. Systemic complications are more common in women, and can include lesions beyond the genitalia, urinary retention, and aseptic meningitis. Primary infection may be distinguished from a recurrent infection with more extensive involvement, lymphadenopathy, and fever. Recurrent infections are typically less severe, and involve three to five vesicles on the genitalia, with resolution in one week.
Wrestlers are prone to extensive involvement when exposed because of pressure contact. It is essential to keep anyone with an outbreak of herpes off the mat. Those athletes with known recurrences should take suppressive dosing of actclovir or Valtrex during season. Be mindful that a "fever blister" is the herpes virus and spread can occur through self-extension or with direct skin to skin contact on any area of skin or mucosa.
Patients with HSV infection present with a highly variable clinical findings. Lesions in primary infections are initially painful vesicles on an erythematous base. They then progress to pustules and/or ulcerations. It is common to see multiple scattered vesicles, most commonly around the mouth and lips in HSV-1. Lesions will typically crust over and resolve within 2-6 weeks. Lesions occurring after the initial infection are typically less severe and fewer in number. It is not necessary for a person to have a known primary outbreak in order for them to have a latent HSV infection, as asymptomatic infection is common.
Genital herpes (HSV-2) usually produces very painful inflammation of the genitalia but may be more pruritic, especially in milder recurrent infections in males. Systemic complications are more common in women, and can include lesions beyond the genitalia, urinary retention, and aseptic meningitis. Primary infection may be distinguished from a recurrent infection with more extensive involvement, lymphadenopathy, and fever. Recurrent infections are typically less severe, and involve three to five vesicles on the genitalia, with resolution in one week.
Wrestlers are prone to extensive involvement when exposed because of pressure contact. It is essential to keep anyone with an outbreak of herpes off the mat. Those athletes with known recurrences should take suppressive dosing of actclovir or Valtrex during season. Be mindful that a "fever blister" is the herpes virus and spread can occur through self-extension or with direct skin to skin contact on any area of skin or mucosa.
 Recurrent facial herpes simplex |
|

Varicella Zoster Virus
Varicella - Fitzpatrick's Dermatology
Varicella zoster virus is the cause of varicella (chickenpox) and herpes zoster (shingles). Varicella is typically symptomatic and occurs in childhood, while herpes zoster is a reactivation of latent varicella infection and will develop in 20 percent of adults and 50 percent of immunocompromised patients. Early detection and antiviral treatment of herpes zoster can reduce or eliminate serious sequelae resulting from the disease. Vaccines are now available for both varicella (Varivax) and herpes zoster (Zostavax), and in turn should change the incidence of both varicella and herpes zoster.
Varicella begins with mild fever, malaise, and myalgia, which is then followed by an eruption of pruritic, erythematous macules and papules. Lesions begin on the face and scalp, then spread to the trunk and extremities. Lesions evolve to vesicles 1-3 mm in diameter with serous fluid surrounded by red halos (dew drops on a rose petal appearance). The presence of lesions in all stages of development is the hallmark of chickenpox. Varicella is usually self-limiting, with secondary bacterial infection of the lesions being the most common complication. Other complications can include CNS complications such as Reye's syndrome, encephalitis, and cerebellar ataxia. In adults, varicella is a more severe syndrome, and pneumonia becomes an important concern, as this untreated pneumonia carries a 10-30 percent mortality rate.
Herpes zoster may occur anytime after varicella infection, but is most common after age 50. It often begins with intense pain, pruritis, tingling, and tenderness. If intense enough, the pain can even be misdiagnosed as a myocardial infarction or appendicitis. In most cases, a painful eruption of vesicles on an erythematous base develops within a sensory dermatome. The most common site of involvement is the trunk, and in some patients the face or extremities may be involved. In children, herpes zoster usually resolves without sequelae. With increasing age or immunocompromised status, complications become more severe, and can include herpetic neuralgia, bacterial infection, scarring, ophthalmic complications, pneumonitis, motor paralysis, and hepatitis. Acyclovir can shorten the duration and severity of this illness, if administered within 24-72 hours after the onset of skin symptoms. If there is involvement of the nasal tip with erythema or lesion, this is an ophthalmic emergency because the eye shares the same innervation.
Varicella begins with mild fever, malaise, and myalgia, which is then followed by an eruption of pruritic, erythematous macules and papules. Lesions begin on the face and scalp, then spread to the trunk and extremities. Lesions evolve to vesicles 1-3 mm in diameter with serous fluid surrounded by red halos (dew drops on a rose petal appearance). The presence of lesions in all stages of development is the hallmark of chickenpox. Varicella is usually self-limiting, with secondary bacterial infection of the lesions being the most common complication. Other complications can include CNS complications such as Reye's syndrome, encephalitis, and cerebellar ataxia. In adults, varicella is a more severe syndrome, and pneumonia becomes an important concern, as this untreated pneumonia carries a 10-30 percent mortality rate.
Herpes zoster may occur anytime after varicella infection, but is most common after age 50. It often begins with intense pain, pruritis, tingling, and tenderness. If intense enough, the pain can even be misdiagnosed as a myocardial infarction or appendicitis. In most cases, a painful eruption of vesicles on an erythematous base develops within a sensory dermatome. The most common site of involvement is the trunk, and in some patients the face or extremities may be involved. In children, herpes zoster usually resolves without sequelae. With increasing age or immunocompromised status, complications become more severe, and can include herpetic neuralgia, bacterial infection, scarring, ophthalmic complications, pneumonitis, motor paralysis, and hepatitis. Acyclovir can shorten the duration and severity of this illness, if administered within 24-72 hours after the onset of skin symptoms. If there is involvement of the nasal tip with erythema or lesion, this is an ophthalmic emergency because the eye shares the same innervation.
|
 Herpes zoster - pectoral area |

Epstein-Barr Virus
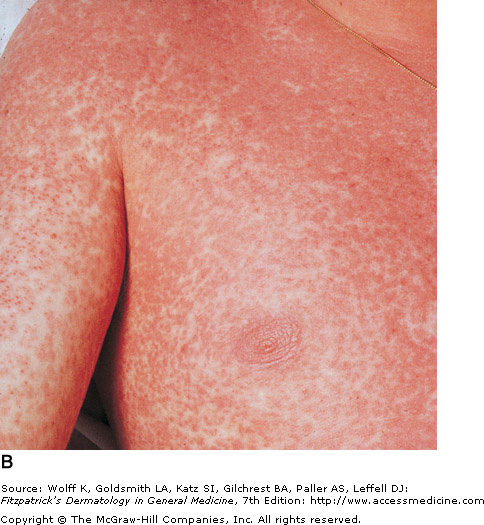
Copper papules after taking amoxicillin
Epstein-Barr virus (human herpesvirus 4) is responsible for infectious mononucleosis, oral hairy leukoplakia, and other disorders. Many dermatologic findings are associated with EBV infection. Of patients with mononucleosis, 70% of those hospitalized and 10% of all patients reported a non-specific erythematous rash. This typically develops on day 4-6 of the illness, and lasts approximately one week. The exanthem first appears on the trunk and upper extremities, then spreads to the face and forearms. Features of the rash are variable, and may be urticarial, vesicular, purpuric, or petechial. Mononucleosis typically resolves within 2-3 weeks, although symptoms of fatigue can persist for longer periods of time.
If am infectious mononucleosis patient was given ampicillin, penicillin, cephalosporins, or amoxicillin, they may develop a skin eruption approximately a week after taking the antibiotic. Copper colored macular/papular eruptions form, becoming confluent over the trunk and extremities. The lesions are often pruritic, and desquamation occurs one weeks later. Patients should stop taking the drugs, and once the infectious mononucleosis resolves, they are free to take the antibiotics in the future. Because the spleen often enlarges with mono, contact sports and other potential impact activities should be avoided until the spleen returns to its normal size.
If am infectious mononucleosis patient was given ampicillin, penicillin, cephalosporins, or amoxicillin, they may develop a skin eruption approximately a week after taking the antibiotic. Copper colored macular/papular eruptions form, becoming confluent over the trunk and extremities. The lesions are often pruritic, and desquamation occurs one weeks later. Patients should stop taking the drugs, and once the infectious mononucleosis resolves, they are free to take the antibiotics in the future. Because the spleen often enlarges with mono, contact sports and other potential impact activities should be avoided until the spleen returns to its normal size.
Cytomegalovirus: HHV-5

Congenital CMV - blueberry muffin baby
While most cases of cytomegalovirus are subclinical, special attention is needed for immunocompromised patients and neonates. In patients with intact immune systems, cytomegalovirus has been described as a mononucleosis-like syndrome, with sore throat, fever, malaise, myalgias, lymphadenopathy, and hepatosplenomegaly. While a rash may occur in a small number of patients, use of ampicillin during the course of the illness leads to a cutaneous eruption in 80-100% of patients (see Epstein-Barr Virus image above).
Congenital cytomegalovirus infection is the leading cause of deafness and mental retardation in the United States, and may also cause jaundice, intrauterine growth retardation, thrombocytopenia, and intracranial calcifications. Erythropoiesis occurring in the skin may present as Blueberry muffin lesions (purpuric paules and nodules), along with petechiae, purpura, and ichthyosis.
Retinitis caused by Cytomegalovirus is the leading cause of blindness in the AIDS population.
Congenital cytomegalovirus infection is the leading cause of deafness and mental retardation in the United States, and may also cause jaundice, intrauterine growth retardation, thrombocytopenia, and intracranial calcifications. Erythropoiesis occurring in the skin may present as Blueberry muffin lesions (purpuric paules and nodules), along with petechiae, purpura, and ichthyosis.
Retinitis caused by Cytomegalovirus is the leading cause of blindness in the AIDS population.
Parvovirus B19

'Slapped Cheek' Appearance of Parvovirus
Human parvovirus B19 is a single-stranded DNA virus associated with many disorders, including erythema infectiosum. Incidence is the highest in the winter and spring, and transmission occurs by respiratory secretions. Erythema infectiosum is most common in children ages 4-10.
The initial skin symptoms consist of a bright red macular erythema of the cheeks with sparing of the nose. Later, a second stage exanthem occurs with erythematous macules and papules forming a lacy, reticulated pattern on the extremities. This rash lasts for approximately 1-3 weeks, and may be exacerbated by sunlight. While arthritis of the joints can occur in approximately 10% of kids, it is far more common to find arthritis/arthralgia in adults acutely infected with parvovirus B19. Joint involvement is self limited, and occurs in 30-60% of adult patients.
The initial skin symptoms consist of a bright red macular erythema of the cheeks with sparing of the nose. Later, a second stage exanthem occurs with erythematous macules and papules forming a lacy, reticulated pattern on the extremities. This rash lasts for approximately 1-3 weeks, and may be exacerbated by sunlight. While arthritis of the joints can occur in approximately 10% of kids, it is far more common to find arthritis/arthralgia in adults acutely infected with parvovirus B19. Joint involvement is self limited, and occurs in 30-60% of adult patients.
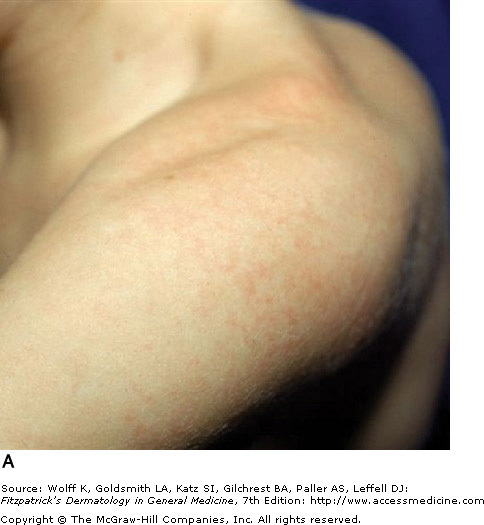 Lacy, reticulated macules and papules on proximal extremities |
 Lacy macules on legs |
