Spirochetes
Lyme Disease

Erythema Migrans - Harrison's Internal Med
Lyme disease is a tick-borne illness caused by the spirochete Borrelia burgdorferi. It affects many organ systems and has characteristic skin findings. Ticks acquire the Borrelia borgdorferi from infected hosts, such as rodents and deer, and inoculate humans through the tick's saliva.
Lyme disease is divided into three stages, each with distinct symptoms and findings. In the first stage, the classic skin manifestation is erythema migrans, which occurs in 50-75 percent of patients. It appears about one week but up to a month after the tick bite, and has two general forms. The first is an expanding erythematous plaque with varying erythema, and second, the classic "bull's eye" or "target" rash of Lyme disease as shown in the picture. The erythema migrans expands centrifugally and ranges in size, anywhere from 4cm x 6cm to a whopping 20cm x 42cm. The lesion will disappear within 2-3 days of treatment, or within one month if left untreated.
Lyme disease is divided into three stages, each with distinct symptoms and findings. In the first stage, the classic skin manifestation is erythema migrans, which occurs in 50-75 percent of patients. It appears about one week but up to a month after the tick bite, and has two general forms. The first is an expanding erythematous plaque with varying erythema, and second, the classic "bull's eye" or "target" rash of Lyme disease as shown in the picture. The erythema migrans expands centrifugally and ranges in size, anywhere from 4cm x 6cm to a whopping 20cm x 42cm. The lesion will disappear within 2-3 days of treatment, or within one month if left untreated.
Syphilis

Chancre of Primary Syphilis - Fitzpatrick's
Syphilis is a sexually transmitted infection caused by Treponema pallidum. It can also be transmitted to infants before birth. Syphilis has primary, secondary, tertiary, and latent stages, all with many different clinical manifestations. Skin manifestations range from genital ulcers to widespread papulosquamous eruptions.
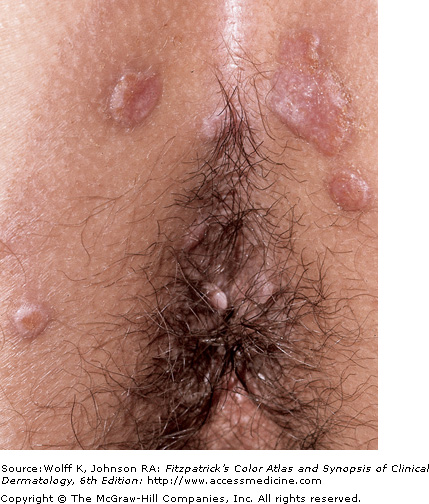
Primary syphilis is classically associated with the chancre. Beginning as a gray-pink macule,10-90 days after exposure,that beomes papular, the chancre develops at the site of inoculation with the formation of a painless erosion, and ulcerates. The chancre is painless and typically occurs on the genitals, perianal area, or the oral cavity, and is self-resolving over time with or without antimicrobial therapy. A person with primary syphilis may never be aware of the lesion. If it is not seen, it will not be noticed.
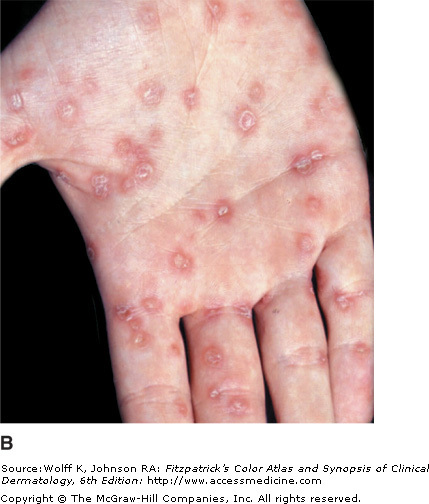
Seconday syphilis occurs 2-6 months after the initial infection, but often 3-12 weeks after the chancre appears. It presents with new skin manifestations. Round/oval macules and papaules 0.5 to 1 cm in diameter, of a pinkish-red to coppery hued in color appear. Later skin eruptions are pustular or acne-like in their appearance. Condylomata lata may also appear as soft, flat-topped, moist, red-to-pale papules, nodules, or plaques. Secondary syphilis is like sarcoid in that its appearance is quite varied. This phase is also quite contagious and may involve the palms, soles, and lips for example, making transfer not only a sexual concern.
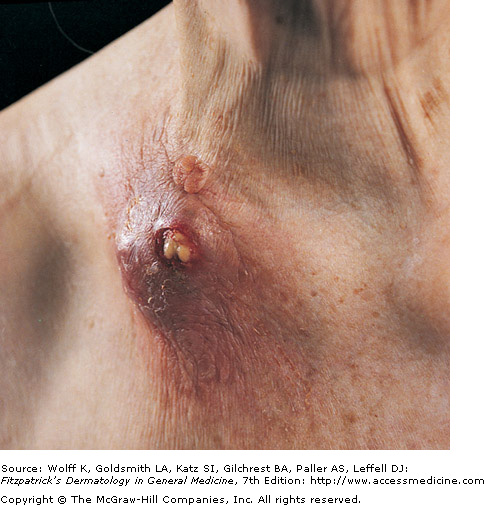
Tertiary syphilis is the final stage, and if left untreated, 15 percent of patients will reach this stage of disease. The main skin lesion of tertiary syphilis is the gumma, which consist of nodular or papulosquamous plaques that may ulcerate. Gummas can occur anywhere on the skin, but are especially prone to the scalp, face, and chest. Gumma lesions commonly occur on bone and respiratory tissues as well. Tertiary syphilis is associated with a host of other symptoms, including neurological dysfunction. Fortunately, the disease is very treatable and cases of tertiary syphilis are relatively rare.
Primary syphilis is classically associated with the chancre. Beginning as a gray-pink macule,10-90 days after exposure,that beomes papular, the chancre develops at the site of inoculation with the formation of a painless erosion, and ulcerates. The chancre is painless and typically occurs on the genitals, perianal area, or the oral cavity, and is self-resolving over time with or without antimicrobial therapy. A person with primary syphilis may never be aware of the lesion. If it is not seen, it will not be noticed.
Seconday syphilis occurs 2-6 months after the initial infection, but often 3-12 weeks after the chancre appears. It presents with new skin manifestations. Round/oval macules and papaules 0.5 to 1 cm in diameter, of a pinkish-red to coppery hued in color appear. Later skin eruptions are pustular or acne-like in their appearance. Condylomata lata may also appear as soft, flat-topped, moist, red-to-pale papules, nodules, or plaques. Secondary syphilis is like sarcoid in that its appearance is quite varied. This phase is also quite contagious and may involve the palms, soles, and lips for example, making transfer not only a sexual concern.
Tertiary syphilis is the final stage, and if left untreated, 15 percent of patients will reach this stage of disease. The main skin lesion of tertiary syphilis is the gumma, which consist of nodular or papulosquamous plaques that may ulcerate. Gummas can occur anywhere on the skin, but are especially prone to the scalp, face, and chest. Gumma lesions commonly occur on bone and respiratory tissues as well. Tertiary syphilis is associated with a host of other symptoms, including neurological dysfunction. Fortunately, the disease is very treatable and cases of tertiary syphilis are relatively rare.
|
 Gumma of Tertiary Syphilis |
Mycobacteria
Leprosy

Leonine Facies of Leprosy
Leprosy is a deforming and disabling chronic infectious disease caused by Mycobacterium leprae. It is slowly progressive, and is associated with an attack on nervous tissue, with preference for the peripheral nerves and skin. There are many subtypes of leprosy, presenting with a broad spectrum of clinical findings.
The form lepromatous leprosy is associated with the least cellular immunity, and initially presents with many poorly defined erythematous macules, papules, nodules, and plaques. The most common sites are the face, buttocks, and legs. Facial lesions can lead to the classic leonine facies (lion-like face). Many post-infection sequelae occur with leprosy, including saddle nose, infiltration of the earlobes, ichthyosis of the lower extremities, and anesthesia of the hands and feet due to peripheral nerve changes.
Tuberculoid leprosy is characterized by few lesions, typically only a few well-demarcated plaques. Some patient may only have neurological symptoms and no skin lesions. Dark skinned individuals will often experience hypopigmentation after the lesions resolve. Leprosy is still a serious medical concern in the developing world and clinicians should closely evaluate travelers and natives to endemic areas.
The form lepromatous leprosy is associated with the least cellular immunity, and initially presents with many poorly defined erythematous macules, papules, nodules, and plaques. The most common sites are the face, buttocks, and legs. Facial lesions can lead to the classic leonine facies (lion-like face). Many post-infection sequelae occur with leprosy, including saddle nose, infiltration of the earlobes, ichthyosis of the lower extremities, and anesthesia of the hands and feet due to peripheral nerve changes.
Tuberculoid leprosy is characterized by few lesions, typically only a few well-demarcated plaques. Some patient may only have neurological symptoms and no skin lesions. Dark skinned individuals will often experience hypopigmentation after the lesions resolve. Leprosy is still a serious medical concern in the developing world and clinicians should closely evaluate travelers and natives to endemic areas.
Tuberculosis

Tuberculosis verrucosa cutis - previously infected
Tuberculosis is a serious infection caused by Mycobacterium tuberculosis that has become even more prevalent throughout the world due to the HIV/AIDS pandemic. Known as one of the great imitators, tuberculosis (TB) can have many clinical manifestations, including cutaneous symptoms.
Skin lesions can be caused by direct innoculation of TB into the skin from an outside source, causing tuberculous chancre, warty tuberculosis, or lupus vulgaris. The tuberculosis chancre forms two to four weeks after innoculation, and evolve from a red papulonodule to an eroding, well-defined ulcer. Spontaneous healing of the chancre will occur in 3 to 12 months. Warty tuberculosis begins as a small, indurated papule with a small ring of inflammation, enlarging over time to form a red-brown verrucous plaque.
Skin symptoms can also occur due to an endogenous infection, presenting with complications such as scrofuloderma, acute miliary tuberculosis, tuberculous gumma, and orificial tuberculosis. Scrofuloderma initially forms as a deep subcuatenous nodule which accumulates inflammatory exudate and necrotic tissue. The nodule drains with secondary ulceration, and bacteria in the draining cold abscess infect the surrounding dermis. The ulcer have a blue border with undermined margins, and multiple ulcers may appear. Miliary tuberculosis has many pin-head sized lesions, made of blue/red papuples with overlying small vesicles. The vesicles can forms crusts with central umbilication, and when they heal, white scars are left behind. The miliary distribution all over the skin is caused by systemic bacteremia. Tuberculous gummas are also caused by bacteremia with cutaneous seeding, leading to a firm subcutaneous nodule that breaks down to form an ulcer. Orificial tuberculosis occurs due to autoinnoculation, and lesions occur in or near an orifice in a patient with advanced TB. Common on the mouth and tongue, lesions are red papules that then ulcerate. The ulcers do not heal spontaneously and can be quite painful.
Skin lesions can be caused by direct innoculation of TB into the skin from an outside source, causing tuberculous chancre, warty tuberculosis, or lupus vulgaris. The tuberculosis chancre forms two to four weeks after innoculation, and evolve from a red papulonodule to an eroding, well-defined ulcer. Spontaneous healing of the chancre will occur in 3 to 12 months. Warty tuberculosis begins as a small, indurated papule with a small ring of inflammation, enlarging over time to form a red-brown verrucous plaque.
Skin symptoms can also occur due to an endogenous infection, presenting with complications such as scrofuloderma, acute miliary tuberculosis, tuberculous gumma, and orificial tuberculosis. Scrofuloderma initially forms as a deep subcuatenous nodule which accumulates inflammatory exudate and necrotic tissue. The nodule drains with secondary ulceration, and bacteria in the draining cold abscess infect the surrounding dermis. The ulcer have a blue border with undermined margins, and multiple ulcers may appear. Miliary tuberculosis has many pin-head sized lesions, made of blue/red papuples with overlying small vesicles. The vesicles can forms crusts with central umbilication, and when they heal, white scars are left behind. The miliary distribution all over the skin is caused by systemic bacteremia. Tuberculous gummas are also caused by bacteremia with cutaneous seeding, leading to a firm subcutaneous nodule that breaks down to form an ulcer. Orificial tuberculosis occurs due to autoinnoculation, and lesions occur in or near an orifice in a patient with advanced TB. Common on the mouth and tongue, lesions are red papules that then ulcerate. The ulcers do not heal spontaneously and can be quite painful.
 Scrofuloderma - Fitzpatrick's Dermatology |
 Orificial Tuberculosis - Fitzpatrick's Dermatology |
